



Preventing Domestic Homicide in Canada: Current Knowledge on Risk Assessment, Risk Management and Safety Planning with Vulnerable Populations
Canadian Domestic Homicide Prevention Initiative with Vulnerable Populations (CDHPIVP) Literature Review on Risk Assessment, Risk Management and Safety Planning
Overall authorship (editors):
Nicole Jeffrey, Jordan Fairbairn, Marcie Campbell, Myrna Dawson, Peter Jaffe, Anna-Lee Straatman
Acknowledgements:
| Research Assistants/Students | ||
|
Abir Al Jamal Danielle Bader Keri Cheechoo Randal David Nichole Faller Meghan Gosse Chelsea Heron |
Nicole Jeffrey Anna Johnson Sakthi Kalaichandran Natasha Lagarde Laura Olszowy Olivia Peters Katherine Reif |
Kayla Sapardanis Mike Saxton Sara Straatman Melissa Wuerch Sarah Yercich |
| Editor | ||
| Jaellayna Palmer | ||
| Graphic Designer | ||
| Elsa Barreto | ||
Suggested Citation:
Jeffrey, N., Fairbairn, J., Campbell, M., Dawson, M., Jaffe, P. & Straatman, A-L. (November 2018). Canadian Domestic Homicide Prevention Initiative with Vulnerable Populations (CDHPIVP) Literature Review on Risk Assessment, Risk Management and Safety Planning. London, ON: Canadian Domestic Homicide Prevention Initiative. ISBN: 978-1-988412-27-6
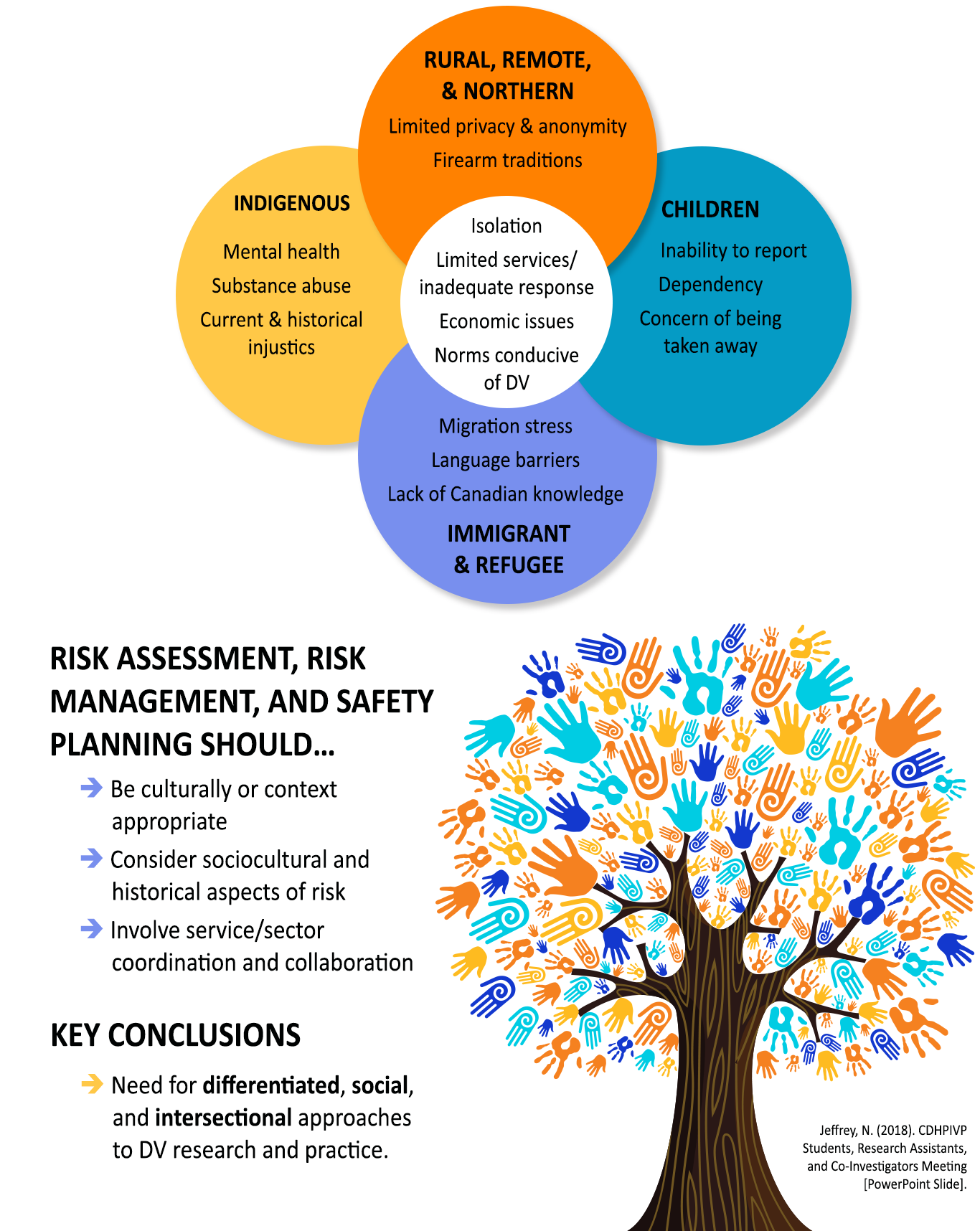
This literature review has identified vulnerabilities for domestic homicide within four specific populations: Indigenous peoples; immigrants and refugees; rural, remote, and northern communities; and children exposed to domestic violence. Although each population can have distinct vulnerabilities for domestic homicide, these populations also share common risk factors for experiencing domestic violence and homicide. To address these vulnerabilities and risks, the literature recommends that risk assessment, risk management, and safety planning be culturally or context appropriate; consider the sociocultural and historical aspects of risk; and involve service/sector coordination and collaboration. Overall, the literature identified a need for differentiated, social, and intersectional approaches to domestic violence and homicide research and practice.
Dear Reader:
This is a living document, which means that it will be regularly updated as new research and/or information becomes available. What you will read here is the result of efforts by the Canadian Domestic Homicide Prevention Initiative with Vulnerable Populations to provide a current and comprehensive assessment of the state of research and common or accepted practices related to domestic homicide and risk assessment, risk management, and safety planning with vulnerable populations. This research literature is voluminous and diverse, posing challenges for identifying and summarizing all the relevant information. We adopted a rigorous approach to identifying and assessing the relevance of literature that is discussed in more detail below. While we have strived to include and capture all relevant material through this process, there is no doubt that we have missed important information, making it crucial that this be considered a living document. As such, after you review the inclusion criteria contained in the methodology section, if you feel we have overlooked information, please let us know. Our goal is to ensure that we ultimately capture all the literature that can be useful to those experiencing domestic violence as well as those working with them to reduce their future exposure.
Contents
Overview of Risk Assessment, Risk Management, and Safety Planning
Risk Assessment, Risk Management, and Safety Planning with Vulnerable Populations
- Indigenous Population
- Rural, Remote, and Northern (RRN) populations
- Immigrant and Refugee Populations
- Children Exposed to Domestic Violence
An Intersectional Review with the Vulnerable Populations
- Immigrants and Refugees
- Indigenous Populations
- Rural, Remote, and Northern Populations
- Indigenous Rural, Remote, and Northern Populations
- Immigrant Rural, Remote, and Northern Populations
- Children Exposed to Domestic Violence
- Intersectional Policy and Practice
- The Need for Differentiated, Social, and Intersectional Approaches
- Priorities for Future Research and Practice
Introduction
Authors: Nicole Jeffrey
Contributors: Jordan Fairbairn
Nationally and internationally, domestic violence is consistently identified as one of the most common forms of gender-based violence and a significant public health problem (Johnson & Dawson, 2011; World Health Organization, 2012, 2016). In rare cases, domestic violence can escalate and result in domestic homicide (Campbell et al., 2003). International and national statistics consistently indicate that women are at greater risk than men of experiencing severe domestic violence and homicide (Burczycka & Conroy, 2017; United Nations Office on Drugs and Crime, 2013). This is also reflected in much of the literature reviewed for this report. Therefore, this report will have a gendered focus with women being survivors/victims of domestic violence and homicide and with men being perpetrators.
This literature review focuses on four populations that experience vulnerabilities for domestic violence and homicide, as well as historical and ongoing factors of marginalization: (1) Indigenous populations; (2) immigrant and refugee populations; (3) rural, remote, and northern populations; and (4) children exposed to domestic violence and homicide. These are not mutually exclusive groups, as individuals may be members of multiple overlapping and intersecting groups. Additionally, these are not the only populations that should be considered vulnerable in the context of domestic violence. Research has identified other marginalized groups who experience vulnerability for domestic violence and homicide including the LGBTQ community (Hansen & Wells, 2015; Loveland & Raghavan, 2014); older women (Sutton & Dawson, 2017; Finfgeld-Connett, 2014); and women with disabilities (Perreault, 2009). However, this literature review represents a starting point to moving beyond general approaches to domestic violence risk assessment, risk management, and safety planning to consider the specific experiences and challenges of various groups.
Why are we starting with these four identified groups? In Canada, Indigenous Peoples and individuals living in rural, remote, and northern communities are at an increased risk of domestic violence and homicide compared to non-Indigenous and urban populations (Northcott, 2011; Statistics Canada, 2006; Statistics Canada, 2016). Immigrants in Canada have lower overall levels of domestic violence compared to non-immigrants. However, this lower risk does not persist when other factors are considered, and the barriers they face may impact their levels of self-reported and police-reported domestic violence (Du Mont & Forte, 2012; Sinha, 2013). These barriers include, but are not limited to, language and cultural differences, which may impact the decision of whether to seek help (Du Mont & Forte, 2012; Sinha, 2013). Little research has examined domestic homicide within immigrant and refugee communities in Canada.
Children may be killed “in the crossfire of a violent altercation” or as an act of revenge against a spouse who leaves an abusive relationship (Jaffe & Juodis, 2006, p. 25; Jaffe, Campbell, Hamilton & Juodis, 2012). In Ontario alone, 29 child deaths occurred in the context of domestic violence between 2002 and 2010 (Office of the Chief Coroner for Ontario, 2015). Therefore, these four populations each experience specific factors that may explain their vulnerability to domestic homicide and challenges to reporting domestic violence and obtaining support. Assessing and managing these factors is crucial for preventing domestic violence and homicide, yet there is a paucity of research identifying these specific risks among these populations and how they might be addressed.
The Canadian Domestic Homicide Prevention Initiative with Vulnerable Populations (CDHPIVP) emerged to help address these noted gaps in research and practice. This Canada-wide initiative seeks to further our understanding of domestic homicide risk among the four vulnerable populations noted above in order to inform risk assessment, risk management, and safety planning. One of the initiative’s main objectives is to conduct cross-sectoral research on risk assessment, risk management, and safety planning to enhance our national capacity to reduce domestic violence and domestic homicide among vulnerable populations.
The present literature review is a first step in that process. The purpose is to systematically and critically review the national and international literature on risk assessment, risk management, and safety planning among the four vulnerable populations. This review provides a current and comprehensive assessment of the state of research and best practices as well as providing a foundation for future research by the CDHPIVP.
Related to these overlapping populations, the research questions we are seeking to answer are: (1) what are the specific risk factors among Indigenous populations; rural, remote, and northern populations; immigrant and refugee populations; and children exposed to domestic violence and homicide; and (2) what risk assessment, risk management, and/or safety planning strategies prevent domestic violence among Indigenous populations; rural, remote, and northern populations; immigrant and refugee populations; and children exposed to domestic violence and homicide?
Overview of Literature Review Report
We begin this literature review with a brief overview of international domestic homicide death review and prevalence, as well as current challenges collecting and sharing data on domestic homicides. We then explain the method for each phase of this systematic literature review, briefly review the theoretical frameworks that guided our analysis of the existing literature, and provide an overview of current domestic violence risk assessment, risk management, and safety planning definitions and research. Next, we provide a comprehensive review of the literature on vulnerabilities, risk assessment, risk management, safety planning, and future priorities for research and practice among the four vulnerable populations (Indigenous populations; rural, remote, and northern populations; immigrant and refugee populations; and children exposed to domestic violence). Finally, we discuss the findings of our literature review and argue for the need for differentiated, social, and intersectional approaches to domestic violence research and practice.
Domestic Homicide
Domestic homicide has been a research focus around the world, including systematic death reviews and inquiries. There are established death review committees in Canada, the U.S., New Zealand, Australia, and the U.K. (Bugeja, Dawson, McIntyre, & Walsh, 2015; Dawson, 2017). Countries around the world with death review committees provide expansive definitions of domestic homicide (Fairbairn, Jaffe, & Dawson, 2017). In Canada, domestic violence death review committees (DVDRCs) expand upon the understanding of domestic homicide as the most extreme form of domestic violence to include victims beyond intimate partners. In Ontario, for example, domestic homicide is defined as “all homicides that involve the death of a person, and/or his or her child(ren) committed by the person’s partner or ex-partner from an intimate relationship” (Office of the Chief Coroner for Ontario, 2015, p. 2).
Domestic homicide is a gendered crime. In Canada, the rate of domestic homicide is 4.5 times higher for female victims than for male victims (Beaupré, 2015). Between 2003 and 2013, police reported 960 intimate partner homicides, with 747 committed against a female victim, representing over 75% of intimate partner homicides (Beaupré, 2015). 76% of domestic homicides involve current or former married and common-law spouses (Beaupré, 2015). Across countries where homicide data are collected, more than one third of homicides of women are perpetrated by an intimate partner (Stöckl et al., 2013). Additionally, one in seven homicides is committed by an intimate partner, with the proportion of women killed by a partner being six times higher than the proportion of men killed by a partner (Stöckl et al., 2013). The gendered nature of these deaths has been reported in multiple countries, including Sweden and Denmark (Rying, 2001; Leth, 2009), England and Wales (Aldridge & Browne, 2003), Finland (Weizmann-Henelius, Matti Grönroos, Putkonen, Eronen, Lindberg, & Häkkänen-Nyholm, 2012), New Zealand and Australia (Family Violence Death Review Committee, 2014; New South Wales Domestic Violence Death Review Team, 2015), the U.S. (Cooper & Smith, 2012), and South Africa (Abrahams, Mathews, Martin, Lombard, & Jewkes, 2013). While much research has looked at prevalence rates and risk factors, less is known about how to best enhance risk assessment, risk management, and safety planning strategies, especially across diverse and vulnerable populations.
Research Challenges
There have been some noteworthy challenges regarding collecting and sharing data on domestic homicides. First, multiple professionals across different disciplines become involved once a homicide occurs, including police, coroners, pathologists, and crown attorneys. As a result, information regarding each case is not located in one specific place or system (New Brunswick DVDRC, 2012). Another concern when involving multiple professionals is the challenges that can occur in terms of communication. For example, when collecting information regarding the victim-offender relationship, information may be missing, partly due to the nature of homicide data and the poor links between police and coroner information, even when advanced homicide monitoring data systems are in place (Stöckl et al., 2013). Some victims may have been isolated and prior violence may have been hidden, which places a demand on police for more thorough interviews with friends, family, neighbours, and co-workers. These challenges further emphasize the importance of (a) establishing and maintaining domestic violence death review committees to ensure collaboration among different sectors when collecting and sharing homicide data as well as (b) developing more innovative research methods to address priority research questions.
Domestic violence victims and perpetrators are not a homogenous population: therefore, how this violence is experienced and prevented is shaped by various intersecting factors including geographical location, socio-economic status, racialization, colonialism, age, and immigration status, among other factors. As this literature review demonstrates, when looking specifically at risk assessment, risk management, and safety planning research in the context of domestic violence, it is important to consider the various intersecting factors. By identifying gaps and challenges in the existing literature, we can begin formulating a knowledge base that can support prevention efforts across diverse and marginalized populations.
The next chapter provides a description of the methodology for the literature review including the search strategy and analysis.
Literature Review Methodology
Authors: Nicole Jeffrey
Contributors: Jordan Fairbairn
This systematic review consisted of three phases: a literature search, annotated bibliographies, and a literature analysis. Two research questions guided this search: (1) what are the risk factors among Indigenous populations; rural, remote and northern populations; immigrant and refugee populations; and children exposed to domestic violence and homicide and (2) what risk assessment, risk management, and/or safety planning strategies prevent domestic violence among Indigenous populations; rural, remote, and northern populations; immigrant and refugee populations; and children exposed to domestic violence and homicide? The first research question was identified as important to understanding domestic violence. The second research question was developed using a PICOS framework (Higgins & Green, 2011); i.e., it specified the types of populations or participants being studied (P), the types of interventions (I), comparisons to other possible interventions (C), the types of outcomes that were of interest (O), and the study designs used to evaluate the effects of the interventions on those outcomes (S). The goal of the review was to synthesize research on risk assessment, risk management, and safety planning related to incidences of repeat or lethal domestic violence among Indigenous populations; rural, remote, and northern populations; immigrant and refugee populations; and children exposed to domestic violence.
Literature Search Strategy
The review was international in scope and included documents written in English and also dated between January 01, 2000 to December 31, 2015[1]. A wide range of academic and grey literature sources were included, such as journal articles, reports, conference papers, theses, and dissertations. We began by developing for each vulnerable population a comprehensive list of search term combinations that included different terms for the intervention, the outcome (i.e., violence), and the population (see Table 1). Research assistants entered each combination of search terms (e.g., prevent* AND “domestic homicide” AND child*) into the ProQuest and PubMed databases.
Table 1: Literature Search Terms
|
The Intervention |
The Outcome (i.e., violence) |
The Population |
|
prevent* |
“domestic homicide” |
Aboriginal |
|
intervention* |
“domestic violence” |
Indigenous |
|
tool* |
“child homicide” |
rural |
|
treatment* |
femicide |
remote |
|
risk* |
filicide |
northern |
|
Safety |
“intimate partner violence” |
immigrant* |
|
|
“murder-suicide” |
refugee* |
|
|
“spousal homicide” |
child* |
|
|
“family violence” |
|
|
|
uxoricide |
|
|
|
“wife assault” |
|
|
|
“wife battering” |
|
To identify relevant documents, research assistants screened all titles and abstracts for a focus on (a) domestic violence; (b) risk assessment, risk management, or safety planning strategies, or identification of risk or vulnerability factors, particularly for the four identified populations; and (c) one or more of the four vulnerable populations (though relevant articles not focused on these four populations were also included). Articles that met the above criteria were added to a shared EndNote[2] library. A total of 1,299 academic references were generated from this process: 187 in the Indigenous group; 215 in the rural, remote, and northern group; 266 in the immigrant and refugee group; 283 in the children exposed group; and 348 in the general population group.
This process was then repeated for grey literature databases including ProQuest Dissertation and Theses, OpenDOAR, and Google as well as targeted searches on agency websites such as Public Health Agency of Canada and Department of Justice Canada. The first 100 results from each search were selected for review. Grey literature retrieved primarily included conference papers, theses and dissertations, government and non-government reports, and handbooks. A total of 981 documents were generated: 168 in the Indigenous group; 254 in the rural, remote, and northern group; 168 in the immigrant and refugee group; 67 in the children exposed group; and 324 in the general population group. Thus, from thousands of articles scanned during the article searches, 2,280 were selected for further review and inclusion in the CDHPIVP EndNote library.
Next, the titles and abstracts of each document were re-read by members of the CDHPIVP literature review team and rated based on the extent to which they provided information on risk assessment, risk management, and safety planning and on characteristics or circumstances of one of the vulnerable populations. If no abstract was available, the document was scanned for relevance. Based on this process, 589 documents were selected for inclusion in the literature review. Table 2 presents the total references reviewed for the annotated bibliographies and full report.
Annotated Bibliographies
Next, members of the team read each document and completed a data form outlining key pieces of information found within each document, including research purpose, theoretical framework, methods, main findings, and any recommendations related to risk assessment, risk management, or safety planning. This information was used to write a summary for each document. The summaries were then compiled into several annotated bibliographies based on the population they pertained to (i.e., Indigenous; rural, remote, and northern; immigrant and refugee; children exposed; or general population). Overlapping articles were included in both relevant annotated bibliographies (e.g., Indigenous and rural, remote, and northern; immigrant and refugee and children).
Table 2: Reference Breakdown
|
Group |
Academic Literature |
Grey Literature |
Total |
|
General risk assessment, risk management, and safety planning |
31 |
25 |
56 |
|
Indigenous |
34 |
48 |
82 |
|
Immigrant and refugee |
117 |
81 |
198 |
|
Rural, remote, and northern |
76 |
58 |
134 |
|
Children |
93 |
26 |
119 |
|
TOTAL |
351 |
238 |
589 |
Literature Analysis
Team members then read and took notes about each document/article for the data collection sheet to summarize the focus and objective of each study, the theoretical approach and methods, the tools, scales or assessment instruments tested, the risk factors identified for the population, and the core findings or recommendations made pertaining to risk assessment, risk management, and safety planning. Following this process, four team members, including two project supervisors, imported these summaries into NVivo (a qualitative analysis software) to code and organize key findings according to: (1) risk assessment, (2) risk management, (3) safety planning, and (4) theoretical frameworks used. Each summary sheet was coded once, and researchers conferred regularly to address questions as they arose. Additionally, as the researchers coded for these core themes they identified additional emerging themes pertaining to barriers to service provision, protective strategies, risk factors, and recommendations for each vulnerable population. The information in each code was then used as a basis for writing up the vulnerable populations chapters.
Theoretical Frameworks
Authors: Nicole Jeffrey, Jordan Fairbairn, Myrna Dawson
Various frameworks are used to understand domestic violence and domestic homicide. In this section, we argue for the importance of the social ecological model for unpacking literature on risk factors, risk assessment, risk management, and safety planning for vulnerable populations; and we explain its use in this literature review. We also outline exposure both reduction and intersectionality as two theoretical lenses that guide the CDHPIVP’s focus on risk assessment, risk management, and safety planning and, in this regard, point to the need to move beyond general strategies to center vulnerable and marginalized populations.
Social Ecological Model
In recent decades, the social ecological model has emerged as a central way to understand gendered violence such as domestic and sexual violence. This model was originally developed by Bronfenbrenner (1979; 2005) to explain “how human beings grow and change in the context of multiple systems” (Nelson & Lund, 2017, p. 12). It was later adapted by others (e.g. Heise, 1998; Dahlberg & Krug, 2002) to lay out various levels of influence (ecologies) to understand complex phenomena such as violence against women (Heise, 1998). In the context of the prevention of violence against women, the social ecological model explores how risk factors occur at individual, relationship, community, and societal levels and targets prevention efforts accordingly (see Heise, 1998; Dahlberg & Krug, 2002).
Although the exact terminology and number of levels vary,[3] the social ecological model is founded on the principle that the origins and consequences of violence involve a combination of factors at multiple levels (Oetzel and Duran, 2004, p. 52). This framework is important because it recognizes the interconnectedness of various risk factors. Additionally, it allows us to integrate individual level theories (e.g. social learning theory) with societal-level theories such as feminist perspectives (Heise, 1998; Johnson & Dawson, 2011). This fills an important gap in the “either-or” approach to individual and societal explanations of violence. As Heise (1998, p. 262-263) explains, “Theorists have either tended to emphasize individual explanations for violence…or they propose social/political explanations…Only recently have theorists begun to concede that a complete understanding of gender abuse may require acknowledging factors operating on multiple levels”
This literature review explores research on domestic violence risk assessment, risk management, and safety planning with vulnerable populations. Because domestic violence has historically been considered a private event, most research has focused on individual level risk factors (Cunradi, 2010). However, in recent years there has been increased and widespread awareness that individual understandings and prevention strategies alone will not eliminate domestic violence. Increasingly, research and policy recognize that addressing domestic violence requires understanding and targeting various levels of prevention (see, for example, Alaggia, Regehr & Jenney, 2012). For example, the Centers for Disease Control and Prevention (CDCP, 2017, para. 3) states that “A combination of individual, relational, community, and societal factors contribute to the risk of becoming an IPV [intimate partner violence] perpetrator or victim. Understanding these multilevel factors can help identify various opportunities for prevention.”
Table 1 Outlines select examples of risk factors at various levels (CDCP, 2017).
Table 1, Examples of risk factors at multiple levels
|
Level |
Risk factors |
|
Individual |
Prior history of being physically abusive; belief in strict gender roles |
|
Relationship |
Dominance and control within the relationship |
|
Community |
Weak community sanctions against domestic violence |
|
Societal |
Traditional gender norms |
Adapted from the Centre for Disease Control and Prevention (2017)
Understanding multilevel factors may be additionally important in working with vulnerable and/or historically marginalized population. For example, Nelson and Lund (2017) explain that
Efforts to support women to safety and out of isolation will not be as effective unless practitioners carefully consider WWD’s [women with disabilities] entire ecological context as a person with a disability and the consequences of reciprocal interactions between these various systems. (p. 11)
Furthermore, as this literature review discusses, Indigenous communities are an example of a historically marginalized population where (a) a focus on individual and relationship level risk factors for domestic violence is insufficient and (b) an understanding of colonization and structural violence is imperative to working on risk assessment, risk management, and safety planning. Thus, the social ecological model can help to move past a focus on individual-level risk factors to understand how communities, families, and societies at-large feature in risk assessment, risk management, and safety planning.
Given the centrality of this framework in current research and practice, this literature review uses the social ecological model as the overarching framework to highlight the complex and multifaceted nature of domestic violence. This understanding is furthered by our use of the theoretical tools exposure reduction and intersectionality, discussed in further detail in the following sections. When understood in combination with the social ecological model, exposure reduction and intersectionality frameworks help emphasize that preventing domestic homicide requires (a) addressing risk factors for each population at multiple levels to reduce exposure to violent relationships and (b) developing risk assessment, risk management, and safety planning strategies at multiple levels that consider overlapping identities and intersecting axes of oppression.
Exposure Reduction Framework
Exposure reduction is a framework emphasizing that domestic homicide prevention requires the identification of mechanisms to support intimate partners in enabling them to reduce their risk of victimization. This may occur by helping them leave an abusive relationship, overcoming barriers that prevent them from protecting themselves in an effective manner, or addressing perpetrator attitudes and behaviours—including making them more accountable (Dawson, Bunge, & Balde, 2009; Dugan, Nagin, & Rosenfeld, 1999, 2001, 2003). This framework has been used to help explain recent declines in intimate partner homicides in the U.S. and Canada (Dawson et al., 2009; Dugan et al., 1999, 2001, 2003). The framework is based on the consistent finding that prior ongoing relationship violence is a major risk factor for intimate partner homicide (Browne, Williams, & Dutton, 1999; Campbell, 1992; Campbell et al., 2003; Gartner, Dawson, & Crawford, 1999; Goetting, 1995).
Thus, resources, policies, programs, and broader social changes that effectively help abused partners to leave an abusive relationship, to reduce their risk by effectively addressing the violence in a relationship, or to prevent these relationships from developing (i.e., exposure-reducing mechanisms) should reduce the rate of intimate partner homicide (Dawson et al., 2009; Dugan et al., 1999, 2001, 2003). Drawing from this framework, this literature review considers risk assessment, risk management, and safety planning strategies that aim to prevent domestic violence from occurring, with the understanding that ending exposure to domestic violence will reduce domestic homicide rates.
Supporting the exposure reduction framework, three broad social changes—and, hence, exposure-reducing indicators—have been linked to declines in intimate partner homicide rates: (1) increased gender equality, such as women’s increased income and educational attainment relative to men’s; (2) changes in the structure of intimate relationships, such as decreased marriage rates; and (3) changes associated with the domestic violence movement, such as increased domestic violence resources (e.g., legal services; Dawson et al., 2009; Dugan et al., 1999, 2003; Reckdenwald, 2008; Reckenwald & Parker, 2010; Rosenfeld, 1997). Each social change supports the idea that, as women become more independent and/or have more opportunities to leave or avoid violent relationships, the likelihood of their being killed by a partner or killing a partner in self-defense is reduced. These links, however, are not always straightforward and sometimes differ based on race/ethnicity, relationship type, and gender. For example, a study by Dugan et al. (2003) in the U.S. found that stronger arrest policies were related to fewer homicides of unmarried partners, but this association was driven largely by African-American victims. Many exposure-reducing mechanisms are also associated with reductions in the rate at which women kill their male partners but not the rate at which men kill their female partners (Dugan et al., 1999, 2003). Dugan et al. (1999, 2003) proposed that this is because women are more likely to kill their partners to protect themselves or their children, and many exposure-reducing mechanisms provide protective alternatives to violence and homicide.
Dugan et al. (1999, 2001, 2003) have also assessed the possibility that, under certain conditions, exposure reducing mechanisms may actually increase the likelihood of intimate partner homicide through a retaliation or backlash effect that might occur if some mechanism or intervention “angers or threatens the abusive partner without effectively reducing contact with the victim” (Dugan et al., 2003, p. 174). For instance, women’s increased economic and/or social status may threaten men’s control in intimate relationships and result in greater violence and homicide as men attempt to regain that control (Dugan et al., 2003; Reckdenwald, 2008). Indeed, Dugan et al. (1999) found that women’s improved economic status was associated with increased female intimate partner homicide victimization. Based on these findings, researchers have concluded that enhanced attention to both victim safety as well as risk management of the perpetrator may be critical in severely violent relationships (Dawson, 2010; Dugan et al., 2003). At the very least, this body of work demonstrates the “clear implications for victims who may not have sufficient access to resources and, as a result, lack one key mechanism for reducing their exposure to further violence” (Dawson, 2010, p. 12).
The exposure reduction framework has not yet been widely tested among diverse and vulnerable populations. However, Chin (2012) found that women’s participation in the labour force was associated with a significant reduction in physical spousal violence in India. Analyzing how economic factors interact with cultural factors, Chin argues that, in a patriarchal cultural setting, increasing financial resources for women without effective exposure reduction (e.g., actual labour force participation) might result in male backlash and negatively impact violence against women. With respect to rural populations, Taylor and Jasinski (2011) suggest that, because many services are located in urban areas, their exposure reducing effects may be less pronounced in rural areas. Thus, more work is needed to better understand the effects of exposure reduction in more diverse and vulnerable populations and how services can better reach these groups.
Intersectionality
Intersectionality (sometimes referred to as interlocking paradigm) is a framework that considers the multilayered dimensions of social identities and/or locations—including gender, race, ethnicity, class, age, ability, geographic location, Indigeneity, sexual orientation, and immigration status—and how they intersect to shape experience (Bograd, 1999; Brassard, Montminy, Bergeron, & Sosa-Sanchez, 2015; Crenshaw, 1989, 1991; Davis, 2008; Erez, Adelman, & Gregory, 2009; Mehrotra, 2010; Sandberg, 2013; Sokoloff, 2008a, 2008b). Despite differences in interpretation and application, many approaches to intersectionality consider the ways that hierarchies of power (and, thereby, oppression) exist along these dimensions (Bograd, 1999). Thus, individual experience (including privilege and oppression) is shaped through the interaction of multiple systems of power. These social locations shape lives in interacting and compounding ways that cannot be captured by looking at each dimension separately (Crenshaw, 1991). Thus, intersectionality moves beyond the traditional research approach of treating each dimension as independent by acknowledging “that the impact of intersecting identities is qualitatively different from the impact of any single identity or the addition of them” (Dill & Zambrana, 2009; Etherington & Baker, 2016, p. 3).
Intersectionality can and has informed theory, research, and practice related to several social issues including domestic violence (Bograd, 1999; Cramer & Plummer, 2009; Etherington & Baker, 2016; Kelly, 2011; Sokoloff, 2008a, 2008b). An intersectional framework challenges the traditional primacy of gendered analyses of domestic violence and promotes an examination of how other social locations may intersect with gender to shape women’s experiences of violence (Crenshaw, 1991; Sokoloff & Dupont, 2005). While extremely useful for facilitating a feminist movement against domestic violence, the traditional approach has been dominated by the voices and experiences of White, middle-class women (Richie, 2000; Sokoloff & Dupont, 2005). Intersectional approaches, in contrast, have been crucial for legitimating the experiences of marginalized women from diverse social locations (Crenshaw, 1991; Sokoloff, 2008; Sokoloff & Dupont, 2005). These approaches have also helped explain the complexity of differences in racial and cultural domestic violence prevalence rates. For instance, the importance of socioeconomic status has been highlighted as a central structural factor related to the higher domestic violence prevalence rates among some groups (e.g., Black and immigrant women; Adams & Campbell, 2012; Sokoloff & Dupont, 2005).
An intersectional approach is essential for both understanding and addressing domestic violence among diverse populations—or example, (a) the intersection of various social locations can influence how domestic violence is experienced and interpreted by women and responded to by others; (b) the barriers that exist to obtaining support and safety; (c) the personal and social consequences of domestic violence; and (d) how interventions functions (Adams & Campbell, 2012; Bograd, 1999; Brassard et al., 2015; Sandberg, 2013; Sokoloff, 2008a, 2008b). Thus, intersectionality providing a more nuanced understanding of the needs and experiences of diverse populations can, in turn, assist in the creation of more relevant, effective, and culturally-sensitive services and policies. Indeed, strategies that are developed based on the experiences of a homogenous group of women or that do not consider how additional axes of oppression shape some women’s lives will be less fruitful for (and potentially harmful to) some groups of women (Crenshaw, 1991; Sokoloff & Dupont, 2005). This may be particularly important in the areas of risk assessment, risk management, and safety planning.
To date, an intersectional approach has been used in domestic violence research and theory development with all of the vulnerable populations of interest in this report including immigrant woman (e.g., Adams & Campbell, 2012; Erez et al, 2009; Sokoloff, 2008; Sokoloff & Pearce, 2011), Indigenous women (e.g., Brassard et al., 2015; Centre de recherché interdisciplinaire sur la violence familiale et la violence faite aux femmes, 2011), and, to a lesser extent, children exposed to domestic violence (e.g., Etherington & Baker, 2016) and women living in rural and remote locations (e.g., Sandberg, 2013). As one example, research finds that intersecting social locations such as gender, ethnicity, and legal status contribute to immigrant women’s domestic violence experiences and barriers to help-seeking. This includes limited access to social service or criminal justice services, legal dependency on their abusers, fear of losing the support of their immigrant communities, isolation, and fear of deportation (Adams & Campbell, 2012; Erez et al., 2009).
Overview of Risk Assessment, Risk Management, and Safety Planning
Authors: Nicole Jeffrey
Contributors: N.Zoe Hilton, Randy Kropp, Marcie Campbell, Jordan Fairbairn
Risk assessment, risk management, and safety planning are key processes in the prevention of domestic violence and homicide. This chapter refers to literature in the field to provide a brief overview of risk assessment, risk management, and safety planning; however, this chapter is meant to provide information and context and was not part of the literature review.
Risk Assessment
Although there is little consensus in the literature with respect to defining risk, most define it in terms of a victim’s likelihood of experiencing or a perpetrator’s likelihood of perpetrating future domestic violence (DV) or homicide (Belfrage, Strand, Storey, Gibas, Kropp, & Hart, 2012b; Campbell et al., 2004; Campbell, Webster, & Glass, 2009; Eke, Hilton, Harris, Rice, & Houghton, 2011; Hilton & Harris, 2009; Hilton, Harris, Rice, Houghton, & Eke, 2008; Hilton et al., 2004; Messing, Campbell, Webster, Brown, Patchell, & Wilson, 2015; Nicholls, Pritchard, Reeves, & Hilterman, 2013). The CDHPIVP defines risk assessment as “evaluating the level of risk of harm a victim (or others connected to the victim) may be facing including the likelihood of repeated violence or lethal (dangerous) violence, based on a professional’s judgment and/or a structured interview and/or a tool (instrument) that may include a checklist of risk factors” (Campbell, Hilton, Kropp, Dawson, & Jaffe, 2016, p. 3). Risk assessment may be carried out by professionals working in different human services. Some of these service providers may be specialists in the domestic violence field (such as police officers and shelter workers); other professionals may be drawn into these issues on an occasional basis, e.g., in workplaces and post-secondary settings (such as mental health professionals, nurses, doctors, corrections staff, and human resources and security personnel). Professionals should strive to determine the most appropriate intervention to manage and mitigate the risk (Kropp, 2008; Nicholls et al., 2013). Thus, the goal of risk assessment is to inform risk management and safety planning to prevent future violence.
There are three main approaches to risk assessment: (1) unstructured clinical decision making, (2) the actuarial approach, and (3) structured professional judgment. In the first approach, professionals in the DV field assess risk more informally, without guidelines, using their own judgment and experience in the field (Campbell et al., 2016; Kropp, 2008; Nicholls et al., 2013). This approach is beneficial in that it can be tailored to each individual case. However, the subjective nature of this approach means it may miss important sources of information and risk factors identified in the literature that could otherwise be used to inform appropriate and effective interventions (Campbell et al., 2016; Kropp, 2004, 2008). Personal preferences, biases, and specialized trainings might also mean that empirically studied and widely accepted risk factors and intervention strategies are disregarded or overlooked (Campbell et al., 2016). Because of this challenge, many in the field are moving away from unstructured clinical decision making and are using more structured approaches to risk assessment (Dutton & Kropp, 2000; Kropp, 2008; Hilton & Harris, 2005).
Secondly, actuarial approaches to risk assessment use a tool containing empirically-derived risk factors, which are combined and interpreted using statistical models to estimate a perpetrator’s risk of (re)offending. Actuarial tools compare an individual perpetrator’s risk to that of other known perpetrators and provide an estimate of the probability of reoffending (Campbell et al., 2016; Nicholls et al., 2013). Two common actuarial risk assessment tools identified in the literature are the Ontario Domestic Assault Risk Assessment Guide (ODARA; Messing & Thaller, 2013; Hilton & Harris, 2009; Hilton et al., 2004) and the Domestic Violence Risk Appraisal Guide (DVRAG; Hilton et al., 2008). Actuarial approaches have greater reliability than unstructured clinical decision making (Grove & Meehl, 1996; Nicholls, Desmarais, Douglas, & Kropp, 2002) and predict violent recidivism with greater accuracy than unstructured risk assessment and structured professional judgment tools (Hilton & Harris, 2005). Actuarial approaches fit within the Risk Need Responsivity (RNR) framework. The RNR framework states that (a) perpetrator recidivism can be reduced if the level of treatment provided is proportional to the perpetrator’s risk to re-offend (risk principle); (b) treatment should focus on dynamic risk factors directly linked to the perpetrator’s violent behaviour (e.g., substance abuse; family/marital relationships; employment) (need principle); and (c) treatment should be about engaging the perpetrator and providing evidence-based interventions that reduce violent/criminal behaviour and tailoring interventions to enhance the perpetrator’s strengths while accommodating for certain barriers (e.g., learning disabilities, motivation, mental health) (responsivity principle) (Bonta & Andrews, 2007; Canales et al., 2013). Within this framework, actuarial approaches can suggest an overall level of risk management that might be needed; however, they do not inform specific management or prevention strategies or allow consideration of contextual or case-specific factors (Douglas & Kropp, 2002; Kropp, 2004).
Finally, the structured professional judgment approach assesses risk using guidelines that reflect theoretical, clinical, and empirical knowledge about DV (Douglas & Kropp, 2002; Kropp, 2004). Common structured professional judgment risk assessment tools include the Spousal Assault Risk Assessment – Version 3 (SARA–V3; Kropp & Hart, 2015; Dutton & Kropp, 2000; Kropp & Hart, 2000; Kropp, Hart, Webster, & Eaves, 1994; Messing & Thaller, 2013) and the Danger Assessment* (DA; Campbell et al., 2009; Dutton & Kropp, 2000; Messing & Thaller, 2013). This approach offers a middle ground between unstructured clinical decision making and the actuarial approach. It is structured in that it provides professionals with guidelines for risk factors, information gathering, and risk management strategies; yet it is flexible and practical in that it allows some professional discretion in determining risk (Campbell et al., 2016; Douglas & Kropp, 2002; Kropp, 2008; Kropp & Hart, 2015). The flexibility of the structured professional judgment approach allows for the inclusion of case-specific factors as well as women’s own perceptions of risk, which can enhance prediction (Heckert & Gondolf, 2004; Stansfield & Williams, 2014; Weisz, Tolman, & Saunders, 2000). However, this flexibility also makes this approach more subjective as the level of risk is based on the professional’s discretion, the qualifications of the professional, and the information provided for the assessment (Helmus & Bourgon, 2011). Some professionals feel uncomfortable with the amount of subjectivity needed to assess risk using the structured professional judgment approach (Canales et al., 2013). Therefore, it is important when using the structured professional judgment approach that the professionals are trained and qualified and that multiple sources of information are used (Helmus & Bourgon, 2011; Kropp & Hart, 2000).
Research evaluating and comparing the various DV risk assessment tools is still in its early stages with “considerable methodological limitations hampering the clinical implications that can be drawn” (Nicholls et al., 2013, p. 148). For example, little research has compared multiple risk assessment measures, used prospective or longitudinal designs, or included victims and collaterals to measure recidivism. Nevertheless, research has tended to find modest predictive validity among the various tools (for reviews see Messing & Thaller, 2013; Nicholls et al., 2013; and Helmus & Bourgon, 2011). Although predictive validity is an important test of efficacy since it measures a tool’s ability to correctly predict future (re)assault, other factors must also be considered when choosing which risk assessment instrument to use (e.g., setting, outcome, skills of the assessor, access to information, cultural appropriateness, or usefulness for risk management; Kropp & Hart, 2015; Messing & Thaller, 2013).
Literature in the field proposes several recommendations around the use of DV risk assessment, four of which are discussed here. First, a structured, reliable, and validated tool or guideline should be used when conducting risk assessments; however, if it is not possible to use an established tool or method then the risk assessment should at least consider empirically or professionally supported risk factors (Campbell, et al., 2016). Second, risk assessment should use multiple methods and sources of information such as interviews with the perpetrator, victim(s), and other informants. This might include family and friends, criminal records, and mental health reports. However, assessments should not consider discriminatory information such as race, ethnicity, or socioeconomic status (Campbell et al., 2016; Dutton & Kropp, 2000; Kropp, 2008; Kropp & Hart, 2015). Third, professionals who conduct risk assessments should receive appropriate and adequate training and education on the use of tools or guidelines (Campbell et al., 2016; Kropp, 2008). Finally, while risk assessment can provide information on the nature, degree, and likelihood of risk, it cannot cover all risk factors and circumstances and, therefore, “should not be used to marginalize or minimize the concerns of those victims believed to be at lower risk” (Kropp, 2004, p. 677). It is also important to incorporate the victim’s perspective into an assessment; however, this information is sensitive and should never be shared with the perpetrator to ensure the victim’s safety (Campbell et al., 2016).
Johnson (2010) argues that risk assessment tools can infringe on women’s dignity and autonomy and urges risk assessment administrators to (1) be transparent regarding the objectives, means, and advantages and disadvantages of lethality assessments; (2) obtain informed consent before conducting assessments and permit women to decline; and (3) engage in woman-centered counselling to determine whether and how women want to use the tools and address the violence. Most importantly, risk assessment must not be considered an end in itself; it is part of a process aimed at preventing domestic violence (Campbell et al., 2016; Dutton & Kropp, 2000; Kropp, 2008; Yang, Wong, & Coid, 2010). As such, it should inform risk management and safety planning.
Risk Management
The CDHPIVP defines risk management as strategies intended to reduce the risk presented by a perpetrator of domestic violence (Campbell et al., 2016) and can include treatment, monitoring, or supervision[4] (Campbell et al., 2016; Juodis, Starzomski, Porter, & Woodworth, 2014; Kropp, 2008). Treatment involves the provision of rehabilitative services including violence interventions (e.g., batterer intervention programs; Babcock, Green, & Robie, 2004; Augusta-Scott, Scott, & Tutty, 2017), mental health and addictions treatment (e.g., individual or group psychotherapy), and training programs to improve interpersonal and anger management skills (Juodis et al., 2014; Kropp, 2008). Monitoring involves surveillance or repeated risk assessment so that management strategies can be adapted (Kropp, 2008). Strategies for monitoring include contacts with the perpetrator and other relevant people, field visits, electronic surveillance, and drug testing. Finally, supervision involves restrictions of the perpetrator’s liberties, such as restricting activities (e.g., curfews, weapons prohibitions) and communications (e.g., with (ex)partner or children) or involuntary incarceration (Juodis et al., 2014; Kropp, 2008). Incarceration is often recommended for high-risk perpetrators (Juodis et al., 2014; Kropp, 2008).
Risk management is often associated with the justice system, but many professionals who are in contact with perpetrators have an opportunity to conduct risk management. For example, general practitioners may be particularly well positioned to engage in risk management strategies, such as making referrals to men’s intervention programs (Hegarty, Forsdike-Young, Tarzia, Schweitzer, & Vlais, 2016). Moreover, risk management should ideally involve cooperation “among a number of different professionals working in different agencies, each with a different skill set and mandate” (Kropp, 2008, p. 214). High-risk management teams are one such approach. For example, Domestic Violence Interagency Case Assessment Teams (ICATs) in British Columbia and Multi-Agency Risk Assessment Conferences (MARACs) in the U.K. are examples of multi-agency (e.g., police, victim services, or child welfare) teams who share information to identify, monitor, and manage high-risk domestic violence cases (Ending Violence Association of BC, 2015; Robinson & Tregidga, 2007). Ultimately, their goal is to develop risk management strategies and increase victim safety (Ending Violence Association of BC, 2015; Robinson & Tregidga, 2007).
Risk management teams often meet regularly and consider the needs of both victim and perpetrator in developing their action plans (Jaffe, Dawson, & Campbell, 2011; Robinson & Tregidga, 2007). Preliminary research has confirmed the benefits of multi-agency approaches, including victims’ feelings of support and reduced violence (Robinson & Tregidga, 2007). While considered a best practice in DV risk management, high-risk management teams are not without challenge (Jaffe, Dawson, & Campbell, 2011). For example, there can be issues associated with (a) collaboration among organizations with different (and sometimes competing) mandates, values, and interests and (b) confidentiality when sharing information between organizations (Jaffe, Dawson, & Campbell, 2011).
As indicated above, risk management can and should be informed by risk assessment. For example, risk management strategies can be aimed at specific risk factors and high-risk individuals can be targeted for more intensive risk management strategies (Dutton & Kropp, 2000; Hilton & Harris, 2005; Kropp & Hart, 2015; Yang et al., 2010). The structured professional judgment risk assessment approach offers a very clear link between DV risk factors and specific management strategies, and it allows for identification of perpetrators’ level of risk (Douglas & Kropp, 2002). Douglas and Kropp (2002) offer a useful overview of risk management strategies that correspond to various risk factors. For example, incarceration, intensive supervision, and violence treatment might be used among perpetrators with past violent behaviour, and crisis counselling, hospitalization, and weapons restriction might be used among perpetrators with recent suicidal or homicidal ideation or intent. Although a few studies link risk assessment and management (see Belfrage et al., 2012b), more research on how DV risk assessment can inform risk management is needed, especially given that effective risk management should target causal risk factors (Kropp, 2008; Yang et al., 2010).
Safety Planning
The CDHPIVP defines safety planning as any strategy to protect both DV victims and those around them (Campbell et al., 2016) and further recommends this be considered one of the highest priorities among professionals working with domestic violence victims and perpetrators (Horton et al., 2014). A “crisis-oriented approach that focuses attention on immediate safety needs,” (Lindhorst, Macy, & Nurius, 2005, p. 331-332)it often involves: (a) providing informational documents to victims, including contact information for local resources; and (b) educating victims regarding specific safety strategies, generally centered around having plans for immediate escape in case of actual or threatened violence at home, in the workplace, or other locations where perpetrators can access victims (Campbell, 2001; Goodkind, Sullivan, & Bybee, 2004; Kress, Adamson, Paylo, DeMarco, & Bradley, 2012; Murray et al., 2015). Some examples of strategies include: (a) having clothing, car keys, and important documents gathered and hidden in case the victim needs to leave quickly; (b) removing weapons from the home; (c) creating an escape plan; and (d) discussing the safety plan with a friend or family member (see Murray et al., 2015 for a review). Safety plans are predominantly developed with victims by social service providers (e.g., violence against women advocates, social workers, and counsellors); others, such as primary care physicians, can also help develop safety plans (especially in rural areas; McCall-Hosenfeld, Weisman, Perry, Hillemeier, & Chuang, 2015). Web- and computer-based safety decision aids are also beginning to emerge (Glass, Eden, Bloom, & Perrin, 2010; Koziol-McLain et al., 2015). These automated tools guide women through risk assessment, help them consider safety-related priorities (e.g., child’s well-being, having resources, maintaining privacy, or feelings for partner), and develop tailored safety plans (Bloom et al., 2014). These cost-effective tools can be used in diverse settings, including welfare offices, community agencies, libraries, and women’s own homes when safe and convenient (Glass et al., 2010; Koziol-McLain et al., 2015). One study found that women who used an online safety decision aid felt less decisional conflict and more supported about their safety than women who engaged in the usual safety planning for domestic violence (Eden et al., 2015).
Safety planning is based on the principles of empowerment and autonomy (Campbell, 2001; Campbell et al., 2016). As such, safety planning discussions should be collaborative, ongoing, and contextualized (Campbell et al., 2016; Horton et al., 2014; Lindhorst et al., 2005; Murray & Graves, 2012). A contextualized approach considers and respects women’s choices, perceptions, and situations—including their risk and protective factors, available resources, children, and the trade-offs of different safety strategies—and works with women to develop safety strategies (Campbell, 2001; Lindhorst et al., 2005; Thomas, Goodman, & Putnins, 2015). However, in situations where there is an imminent risk of harm or lethality, the overall safety of the victim and children may take precedence over ensuring the victim has choices and autonomy when developing a safety plan.
Although empirical research on formal safety planning is limited (e.g., Eden et al., 2015; Glass et al., 2010; Goodkind, Sullivan, & Bybee, 2004; Horton et al., 2014; Koziol-McLain, 2015; Kress et al., 2012; Messing, O’Sullivan, Cavanaugh, Webster, & Campbell., 2016; Murray et al., 2015; Thomas et al., 2015). However, studies examining the effectiveness of women’s use of various protective strategies may provide insight. For example, certain formal help-seeking strategies (such as staying in a shelter) appear to improve women’s safety and reduce abuse (Goodkind et al., 2004; Messing et al., 2016). In contrast, fighting back physically and obtaining defensive or security devices (e.g., mace or locks) appear to make the situation worse for many women and may even increase abuse or stalking (Goodkind et al., 2004; Messing et al., 2016). That is, fighting back physically might anger an abuser, and security devices may not deter stalking because stalking can occur from a distance (Goodkind et al., 2004; Messing et al., 2016). This body of work generally supports the importance of DV services and shelters (Goodkind et al., 2004).
This broad risk assessment, risk management, and safety planning literature review provides an overview of various tools and processes for reducing risk for domestic violence and homicide. Despite this important work, individual experiences of risk for domestic homicide are impacted by diverse factors such as racialization, experiences of colonial violence, immigration status, age, and geographical location. As such, the next sections of this literature review consider existing work on risk assessment, risk management, and safety planning specific to the four vulnerable groups: Indigenous populations; children; rural, remote, and northern populations; and immigrants and refugees.
Risk Assessment, Risk Management, and Safety Planning with Vulnerable Populations
The next four chapters provide a summary of the literature on domestic violence risk assessment, risk management, and safety planning with the four vulnerable populations that are the focus of this review. It is important to note that the introductions of each chapter include literature that was not identified in the review to provide an overall context. The literature from the review is summarized and discussed in the key findings and the priorities for research, practice, and policy development.
Indigenous Population
Authors: Olivia Peters, Jane Ursel, Claudette Dumont-Smith
Contributors: Josie Nepinak, Anna-Lee Straatman, Jordan Fairbairn
The term Indigenous[5] is defined by CDHPIVP as an inclusive term to encompass all Indigenous peoples and identities—including status, non-status, Indian, Aboriginal, Native, First Nation, Métis, and Inuit—who live on- or off-reserve. Historically, Indigenous peoples have been subject to colonization, Indian Residential Schools, and massive child apprehensions known as the sixties scoop. As a result of this history of abuse and forced assimilation, Indigenous people across Canada have been marginalized and deeply disadvantaged. One consequence of this history of repeated trauma to Indigenous families and communities is the overrepresentation of Indigenous people as victims of violent crime.
The 2014 General Social Survey (GSS) on Victimization reports that the overall rate of violent victimization for Indigenous people is more than double that of non-Indigenous people (163 per 1,000 versus 74 per 1,000). Indigenous people are more than twice as likely (9%) to report being victims of domestic violence than non-Indigenous people (4%). Indigenous women are especially vulnerable. According to Boyce (2016), their rate of violent victimization (220 per 1,000 people) has been double that of Indigenous men (110 per 1,000), almost triple that of non-Indigenous women (81 per 1,000), and more than triple that of non-Indigenous males (66 per 1,000), (Boyce, 2016). Statistics Canada consistently indicates the overrepresentation of Indigenous women and girls as victims of physical assault, sexual assault, and non-spousal homicide. They are more likely to experience violence or sexual victimization, and they are more likely to be killed by a stranger than non-Indigenous women (Lant, 2014; Native Women’s Association of Canada [NWAC], 2010; Royal Canadian Mounted Police [RCMP], 2015). A destructive stereotype of violence and Indigenous women is the narrative of Indigenous women living high-risk lifestyles. This narrative serves to normalize the violence, blame the victim, and must be deconstructed (Assembly of First Nations, 2013). Indigenous women are often at-risk not because they choose to take risks but because poverty and inadequate services put them at-risk (Federal-Provincial-Territorial Ministers Responsible for Justice and Public Safety, 2016). For example, the infamous “highway of tears,” the only highway between Prince George and Prince Rupert, has no public transport. Between 1969 and 2011 there are 16 known Indigenous murder victims and potentially 40 missing women who are likely victims on this deadly stretch of highway. Similarly, poverty and discrimination result in Indigenous people living in neighbourhoods that are often not safe. Simple daily activity like walking to a bus stop exposes women to risks. They do not choose a lifestyle that is risky; poverty imposes risks.
Statistics and circumstances such as these contribute to the recognition of Indigenous peoples as a particularly marginalized population. As such, part of this project is to map out existing research on preventing domestic homicide and that focuses on Indigenous populations. As this section will highlight, current research on Canadian Indigenous populations and domestic violence tends to focus on risk assessments rather than risk management and safety planning, thus reflecting a paucity of research in these areas.
Recognizing the multiple types of violent victimization that Indigenous people face in Canada, this initiative focuses on violence within the context of current or past domestic relationships. This is not to diminish or minimize the importance of non-domestic violence and homicide perpetrated by non-Indigenous perpetrators against Indigenous women. Rather, the CDHPIVP aims to address a related part of the larger problem of violence against Indigenous people seen both in Canada and around the world. This study deals specifically with risk assessment, risk management, and safety planning strategies for domestic violence and domestic homicide in Indigenous populations.
Indigenous peoples are vastly overrepresented in homicide statistics. Rates of homicide for Indigenous women have remained stable from the year 1980 to 2014 while rates for non-Indigenous women have declined (Miladinovic & Mulligan, 2015). A higher proportion of Indigenous than non-Indigenous people have been killed by someone they know, including intimate partners and other family members (Miladinovic & Mulligan, 2015).
Unique historical circumstances have played a central role in current issues around domestic violence and Indigenous peoples (see subsequent section “Historical Context”). Indigenous populations are more likely to experience concurrent risk factors such as substance abuse, poverty, and a history of physical or sexual abuse (Bottos, 2007). As well, there is a lack of Indigenous-specific supports, Indigenous community resources, and effective alternatives to mainstream justice responses. The preponderance of risk factors among Indigenous people are typically met with mainstream responses considered inappropriate for the needs of their families and communities (Cripps, 2007; Bopp, Bopp & Lane, 2003; Brown & Languedoc, 2004).
The “cultural appropriateness” of responses is a widely-contested topic requiring further examination because it seems to imply a homogeneity among Indigenous communities which are, in fact, much more likely to vary substantially in their needs and in their capacities (NWAC, 2011). There are considerable cultural differences and distinctions both between and within Indigenous communities across Canada. Acknowledging these differences, Indigenous and non-Indigenous researchers, service providers, and other professionals explain that responses to domestic homicide should be specific to the communities in which they work. The uniqueness of and within Indigenous populations requires service responses based on local knowledge and sensitivity to community dynamics.
Acknowledging the statistics and concerns noted above, the literature reviewed calls for more attention and resources for marginalized Indigenous populations across Canada. The CDHPIVP seeks to address these issues and bring Indigenous populations to the forefront of homicide prevention research. Our objectives are to identify what risk assessment, risk management, and/or safety planning strategies might prevent domestic violence in Indigenous communities with attention to the unique historical context and current circumstances of Canadian Indigenous populations.
Indigenous peoples face many unique factors and additional challenges when examining the issue of domestic violence and abuse. Prior to contact, Indigenous peoples had their own governance models, and these varied by nation, spirituality, and cultural beliefs and practices. Through colonialism, Indigenous peoples were forced to accept foreign religious practices and beliefs, governance styles based on a patriarchal system, and laws that were imposed on them. Indigenous peoples, who had been self-governing for hundreds of years, were made ‘wards’ of the government through these colonial actions.
The Indian Act of 1876 (Indian Act, R.S.C., 1985, c. I-5) is specifically a colonial policy that has had a negative impact and continues to discriminate and oppress First Nations. The establishment of Indian Residential Schools, which were disastrous and destructive for Indigenous peoples, ensued from the powers vested under the Indian Act. The primary purpose of these institutions was to assimilate Indigenous peoples within the mainstream population. Records indicate that 150,000 Indigenous children—First Nations, Inuit, and Metis—as young as five were forcibly removed from their parents and communities and forced to attend these state and church-run schools. These schools operated from the mid-1800s, with the last Indian Residential School closing in 1996 (Schwartz, 2015). Former Prime Minister Paul Martin and Supreme Court Chief Justice Beverley McLachlin have described the Indian Residential School experience as “cultural genocide.” Genocide—defined as an attempt to destroy a people, in whole or in part—is a crime under international law (Fine, 2015).
Numerous reports and national studies describe the sexual, physical, emotional, mental, spiritual, and cultural abuses that were inflicted on a great number of Indigenous children attending these schools. Sadly, for some children this went on for years; and, in many instances, multiple generations of a family attended Indian Residential Schools and were victims of various forms of abuse. These traumatic experiences, when left untreated, were and continue to be passed on intergenerationally (Grau & Smith, 2011). Unresolved trauma can manifest itself in destructive behaviours to self, the family, and the community and can result in depression, anxiety, addictions, family violence, and suicidal and homicidal thoughts (Bohn, 2003; Moffitt et al., 2013).
Furthermore, First Nations women were especially affected by the Indian Act. Their “Indian” status was removed upon marrying a non-Indigenous person, unlike their male counterparts whose non-Indigenous spouses gained status upon marriage. This policy made First Nations women subordinate to First Nations men. In 1985 some changes to the Indian Act were legislated to enable First Nations women to re-gain their “Indian” status. However, their offspring have yet to attain equality to that of the descendants of First Nations men; thus, they are still regarded as inferior to their male counterparts.
Indigenous populations have had a long and complicated history of oppression, prejudice, and colonization in North America (Bohn, 2003). In Canada, this history can be traced back to the Indian Act of 1876 that took effect soon after Canada became an independent country in 1867. Through the Indian Act, the traditional ways and practices of Indigenous people and their languages, family and community networks, ceremonies, and territories were taken, destroyed and/or outlawed. The effects are still seen today.
Key Findings for Risk Assessment with Indigenous Peoples
Risk Factors. Statistics indicate that Indigenous peoples live in conditions well below the Canadian average. Many Indigenous peoples, because of their location, (a) live in poverty due to the absence of economic opportunities and the high cost of living; (b) live in sub-standard and over-crowded housing; and (c) have limited social and health supports and services (Moffitt, Mauricio, Marshirette & Mackenzie, 2013). Indigenous peoples, regardless of where they live, are subject to racism and discrimination in the social, health, and justice systems and have limited or no access to culturally-specific and culturally-safe health and social services (Wells, Strafford & Goulet, 2011). Further, Indigenous people are hesitant to access mainstream services because of stereotyping and racism. The barriers experienced by Indigenous peoples are further compounded by residence in rural, remote, and northern communities. Residents in these communities face geographic and transportation barriers to accessing necessary services for a wide range of needs including medical care, police response, addictions, and mental health services.
The negative impacts of colonization and the outdated discriminatory policies that are still in place continue to negatively impact the lives of Indigenous peoples. Rates of stranger violence, domestic violence, self-harm, and substance abuse are higher in the Indigenous population in comparison to the mainstream.
The literature suggests that, as a result of high levels of victimization, it is crucial to restore missing elements of Indigenous culture to address the problem of domestic violence (Blagg, Bluett-Boyd, & Williams, 2015; Brownridge, 2003). Furthermore, strategies to address domestic violence should be holistic in nature and consider the victim’s family and community. A factor that is unique to Indigenous populations concerning domestic violence is the idea of “community dimension” (Bopp et al., 2003). According to Bopp et al. (2003), mainstream responses to domestic violence often emphasize the individual or a specific family rather than the whole community. These authors note that it is important to consider the role of the community in domestic violence research and interventions, and to recognize that Indigenous communities cannot be approached with mainstream models of service. With this in mind, strategies to address domestic violence must be community-specific and developed with local knowledge and an understanding of community dynamics (Bopp et al., 2003).
Comparatively, Indigenous women are at a greater risk of experiencing domestic violence than non-Indigenous women. Indigenous women are more likely to experience violence of all severity levels, with an even greater likelihood of experiencing the more severe forms of violence (Brownridge, 2003; Nicholls, 2008). Brownridge (2008) found that colonization plays a large role in Indigenous women’s elevated risk of experiencing violence. Typically, risk factors do not account for this elevated risk (Brownridge, 2008). Thus, risk of victimization for Indigenous women is increased due to colonization, displacement, and loss of identity and traditional culture (Grau & Smith, 2011).
Factors that are associated with increased risk of violence for Indigenous peoples are poverty, young age, geographic isolation, living common-law, unemployment, low educational attainment, and substance abuse (Brassard et al., 2015; Brownridge, 2003; Burkhardt, 2004; Daoud, Smylie, Urquia, Allan & O’Campo, 2013; Jones, Masters, Griffiths, & Moulday, 2002). In addition, intergenerational trauma resulting from the Indian Residential School experience also places Indigenous peoples at an increased risk for domestic violence. This trauma, when untreated, is passed on from generation to generation and results in destructive behaviour within the family and community (Brownridge, 2003).
Risk Assessment Tools. The importance of using risk assessment instruments that are culturally-informed (designed with Indigenous populations and communities in mind) is found throughout the risk assessment literature. Specifically, risk assessments used with Indigenous populations should not be standardized intervention tools. These tools often neglect the specific needs of Indigenous communities, the role of Canada’s colonial history, and the importance of cultural and community values such as non-verbal communication strategies and Indigenous identity (Amellal, 2005; Buchanan, 2009). The diversity within and between Indigenous communities is not captured in mainstream risk assessment tools. Instead, research indicates that using holistic traditional practices that address and treat anger management, loss of identity, and experiences of trauma and abuse are effective practices among Indigenous populations (Amellal, 2005; Riggs, 2015; Victorian Indigenous Family Violence Task Force, 2003).
Several standardized risk assessment tools are currently used and are discussed in general risk assessment literature. These include, but are not limited to, the Spousal Assault Risk Assessment Guide (SARA), the Ontario Domestic Assault Risk Assessment (ODARA), the Aid for Safety Assessment Planning (ASAP), and the Physical Aggression Couples Therapy (PACT) tool (Al-Yaman, Doeland, & Wallis, 2006; Cairns & Hoffart, 2009; Riel, 2013). In general, these instruments tend to be more generic and are not developed specifically for use with Indigenous populations. For example, Buchanan (2009) found that the predictive accuracy of the Ontario Domestic Assault Risk Assessment (ODARA) and DVSI-R is comparatively weak with Indigenous populations, likely due to a lack of culturally-specific risk factors.
In discussing risk, we must acknowledge the diversity within and between Indigenous communities. For example, while the Danger Assessment has been applied to Indigenous women, Cairns and Hoffart (2009) recommend that the Indigenous women would benefit from an approach to risk assessment that considers the diversity within Indigenous populations. Very few risk assessment tools have been developed for Indigenous peoples; however, those that do exist are often specific to the community. For example, in Alberta a risk assessment has been developed called the Walking the Path Together POP TARTS tool: Protection, Options, Planning: Taking Action Related to Safety (The Alberta Council of Women’s Shelters, 2012). This tool, developed specifically for women living on-reserve, is an alternative to standard safety planning available on-reserve. It provides guidelines for assessing risk, helps women and their children to recognize dangerous situations and behaviour, and encourages women to trust their own feelings, body sensations, and intuitions (The Alberta Council of Women’s Shelters, 2012).
Another example of a resource that may be used when assessing risk with Indigenous peoples is a resource cited in Pimatisiwin (Chase, Mignone & Diffey, 2010) called the Life Story Board. Originally developed for children living in war zones, the Life Story Board allows an individual to create a visual representation of their story in a variety of contexts including violence. Chase, Mignone, and Diffey (2010) explain that the Life Story Board may be useful when assessing the risk of domestic violence, not only for adults but also for children and youth of diverse cultures. To consider the applicability of the Life Story Board within Indigenous communities, the authors conducted research with an Aboriginal Focus Program for social work students and asked Indigenous students to reflect on how the Life Story Board could be used. Responses included: (1) the impact of residential school experiences, (2) experiences with violence and loss, and (3) individual’s sources of strength (Chase et al., 2010). As many Indigenous cultures are characterized by traditions of storytelling, the Life Story Board may be beneficial and widely applicable in that it offers both verbal and nonverbal means of expressing one’s story across languages and levels of literacy (Buchanan, 2009; Riggs, 2015; Bopp et al., 2003; Chase et al., 2010).
Role of Community Professionals. Overwhelmingly, literature on domestic violence program development and delivery recommends that community professionals use a restorative approach that is both culturally-located and -informed. This includes maintaining a strong connection to Indigenous cultures, working with traditional knowledge holders such as Elders, and involving the community when possible (Brown & Sue, 2004). Community professionals working within mainstream agencies (such as social workers, nurses, and doctors) must be sensitive to the needs of Indigenous clients and trained in cultural sensitivity (Davis & Taylor, 2002; Holder, 2015).
Spiwak (2004) identifies the need t to improve and increase education on domestic violence and abuse for caregivers and support workers who work with Indigenous populations. Community professionals must also recognize signs of exposure to domestic violence among children and youth. Victims of violence can play an important role in educating mainstream professionals through workshops with these professionals addressing the social and historical context of their abuse and the cultural context of their healing (Spiwak, 2004). This education can extend beyond the training of community professionals to raising public awareness of the needs and experiences of domestic violence survivors. This not only improves the quality of service from professionals but also can become an essential component of a victim’s healing process (Spiwak, 2004).
It is important for a victim’s voice to be heard in a manner that facilitates his or her healing, educates the public, and is not exploitive. Community professionals working in mainstream agencies, primarily with Indigenous populations must ensure that Indigenous peoples are involved in all levels of program development, implementation, and evaluation (Zellerer, 2003). Specifically, Zellerer (2003) asserts that the use of a holistic approach, in which mainstream methods and traditional Aboriginal approaches are combined, is an effective foundation for programs. Specific recommendations regarding professional conduct include empowering abused mothers, modifying research protocols in cases where Elders are considered the ultimate authority, and maintaining confidentiality in rural, remote, and northern communities (Nixon, Bonnycastle & Ens, 2015; Pauktuutit Inuit Women’s Association, 2005; Puchala, Paul, Kennedy, & Mehl-Madrona, 2010; Davis & Taylor, 2002).
System Collaborations. Criminal justice and health care systems are two major institutional systems that are particularly significant for intervention and treatment in domestic violence cases. The literature provides important findings on collaborations within these two mainstream systems.
The Criminal Justice System
In a comparative analysis of Australia, Canada, and New Zealand, Marchetti and Anthony (2016)* identify legal strategies adopted by mainstream courts to facilitate collaboration with Indigenous peoples. These strategies include) sentencing directives and court accommodations. Sentencing directives require judges to consider as mitigating factors or opportunities for creative and restorative sentences the history of colonialism, displacement, and residential schools (R. v Gladue, 1999) and features of the accused’s background which contributed to the offense. Court accommodations include community representative and Elders in considering sentencing options. These accommodations are identified variously as Circle Sentencing in Canada, Indigenous Sentencing Courts (ISC) in Australia, and Rangatahi Youth Courts in New Zealand.
In Australia, Indigenous sentencing courts, particularly the involvement of Elders and Community Representatives within these courts, play an important role in risk management, leading to lower rates of domestic violence re-offences among Indigenous men (Marchetti & Anthony, 2016). In Canada, an impact study of Circle Sentencing or community-based justice programs concluded that these programs provided culturally-relevant alternatives for Indigenous populations (Department of Justice Canada, 2011).
Along with court innovations, correctional services across Canada have attempted to incorporate Indigenous Elders and practices as options for Indigenous offenders in institutional and community settings. In some jurisdictions, there are specific Indigenous treatment programs for offenders (Department of Justice Canada, 2011). In cities such as Winnipeg with a high urban Indigenous population, there are several Indigenous agencies that offer culturally-specific treatment programs for individuals dealing with their abusive behavior. For example, Ma Mawi Wi Chi Itata, a family centre in Winnipeg, provides the program ”Spirit of Peace” with separate groups for men, women, and children who are dealing with violence in their homes.Literature on system collaboration asserts that services must be sufficiently flexible and responsive to Indigenous populations.
Health Care System
Within the health care system, the inclusion of culturally-relevant and traditional practices can help to reduce domestic violence within Indigenous communities. For example, Puchala et al. (2010) suggest that including traditional spirituality through Traditional Healing Elders in psychiatric practice is effective for reducing domestic violence. The authors used the My Medical Outcomes Profile 2 scale, a patient-generated and individualized tool allowing patients to indicate problems they are most want to address and to set their own treatment goals. This tool indicates severity scores based on the patient’s responses. The authors found that Elder involvement in psychiatric practice had a significant impact on decreasing symptom severity scores from the My Medical Outcomes Profile 2 scale, leading to the finding that Elder involvement is more effective than conventional clinical care.
As previously mentioned, the use and integration of traditional resources and spiritual ceremonies in domestic violence treatment have a significantly positive impact on domestic violence victims and perpetrators (Copenace, 2000; Puchala et al., 2010; Wells et al., 2011). Of these ceremonies and practices, storytelling within the context of the health care system aids in the reconstruction of self-narratives and the redefining of gender relationships (Puchala et al., 2010). As a guiding principle, those working with victims who reach out for support should inform their practice with cultural sensitivity (Community Legal Information Association of Prince Edward Island, 2010).
Key Findings in Risk Management with Indigenous Peoples
The literature on risk management within Indigenous communities largely focuses on the importance of domestic violence intervention strategies that include culturally-competent environments, culturally-relevant interventions, and those which emphasize tradition, honesty, holism, humility, and spirituality as markers of success. Therefore, programs based on traditional values of Indigenous culture are an essential part of protecting and preventing violence against Indigenous women and girls (Federal-Provincial-Territorial Ministers Responsible for Justice and Public Safety, 2016). Further, combining spirituality with everyday life is found to complement existing programs designed for risk management within Indigenous communities (Kiyoshk, 2003). For example, there is evidence that the inclusion of traditional Indigenous teachings, practices, and ceremonies—such as using the Medicine Wheel, smudging, talking circle, and sweat lodge purification ceremonies—has had a positive impact on perpetrators and victims of domestic violence within various contexts (Lester-Smith, 2012; Puchala et al., 2010; Thibodeau & Nixon, 2013). Such traditional and spiritual practices were also found to complement existing programs for perpetrators of domestic violence (Kiyoshk, 2003; Thibodeau & Nixon, 2013; Zellerer, 2003).
Most of the literature mentions the importance of having Indigenous men enter programs or treatment centres for domestic violence that are facilitated by other Indigenous people (especially Elders; Burkhardt, 2004). This is due to the fear of rejection, misunderstanding, and condescension, which Indigenous perpetrators of domestic violence report experiencing in mainstream programs. Specifically, best practices identified for prevention models to manage risk of domestic violence within Indigenous populations include: (1) involve Indigenous staff in the planning, delivery, and evaluation of offender programming; (2) train Indigenous and non-Indigenous workers in regular and ongoing cultural awareness training; (3) provide the option of Indigenous-specific treatment for offenders; (4) include the use of Traditional Healing Elders; and (5) provide the option of involving the family at a later stage in the offender’s treatment process (Bopp et al., 2003; Burnette, 2014; Day et al., 2012; Jones et al., 2002; Puchala et al., 2010; Riel, 2013; Shea, Nahwegahbow, & Andersson, 2010; Spiwak, 2004; Zellerer, 2003). Additionally, intervention programs for family violence in Indigenous communities should focus on healing for the whole community (Burkhardt, 2004).
Risk management literature also highlights how structural inequities such as economic dependency, overcrowding, poverty, lack of health and social services, and poorly funded education increase risk and must be considered in risk management. In addition, experiential factors such as the impact of Indian Residential Schools and intergenerational trauma must be incorporated in risk management programming (Brownridge, 2003; Assembly of First Nations, 2013; Grau & Smith, 2011; Riggs, 2015; Riel, 2013; Riel et al., 2014a; Puchala, et al., 2010). Therefore, important strategies to reduce the risk of domestic violence for Indigenous populations include creating opportunities for economic prosperity, increasing community education, involving elders, providing better availability of family violence prevention and legal services, and providing more services for women and girls in isolated communities (Victorian Indigenous Family Violence Task Force, 2003).
Another significant finding in the literature is that stigma and denial of domestic violence is strongly associated with the high rates of violence (Brown & Sue, 2004). An important component of community education is to give voice to these issues, to challenge stigma and denial, and to identify strategies for intervention. Education that identifies strengths and capacities in the community to overcome violence would enhance prevention efforts (Brown & Sue, 2004; Yuan, Belcourt-Dittloff, Schultz, Packard, & Duran, 2015). Specifically, Davis and Taylor (2002) recommend focusing on teaching younger generations about respect and the consequences of domestic violence as an important prevention method. Because the destruction of traditional practices and language contributed to the dismantling of Indigenous communities, promoting respect for traditional practices, languages, and access and emotional connection to land must be considered an important component of risk management (Assembly of First Nations, 2013; Riggs, 2015). These practices help the offender to connect with their spirituality and to develop respectful relationships with Elders and family members (Thibodeau & Nixon, 2013).
Compared to rural, remote, and northern communities, urban areas have better access to social services, shelters, healthcare, and police interventions. However, even within the urban context, few culturally-appropriate services exist. Attention must be given to the development and inclusion of culturally-appropriate services in an urban context to meet the needs of Indigenous peoples.
For many urban Indigenous women, there are barriers to accessing land and ceremonial resources. However, in response to this need, some urban agencies have facilities on the land and use them for conducting cultural ceremonies and gathering medicines. For example, Ma Mawi Wi Chi Itata Centre has a number of facilities outside of the city of Winnipeg which offer programs for Aboriginal men, women, and children and that include ceremonies, sweat lodges, and medicine gathering opportunities.
In summary, risk management literature emphasizes that initiatives should be based on traditional values of Indigenous culture. Examples of culturally-specific tools and models include (1) Community Holistic Circle Healing process (Cripps & McGlade, 2008), (2) Change of Seasons treatment model (Kiyoshk, 2003), (3) Warriors Against Violence Society (Lester-Smith, 2013), (4) The Kizhaay Anishinaabe Niin (Lamontagne, 2011), and (5) Kanawayhitowin (Taking Care of Each Other’s Spirit Initiative; Lamontagne, 2011).
Key Findings in Safety Planning with Indigenous Peoples
The first part of this section discussed the importance of a community dimension to safety planning, concluding that the vast majority of literature on safety planning focuses on the individual rather than the community. However, the community dimension does appear when referring to specific obstacles Indigenous communities may face for safety planning. For example, Lamontagne (2011) notes that we must be cognizant of the unique situation facing Indigenous women in the North, where women seeking safety are often forced to leave their communities, families, and support networks for extended periods of time. Informal community supports are more likely to be a primary aspect in an individual’s safety planning, particularly in rural, remote, and northern communities and/or for mothers living with abuse (Nixon et al., 2015). As such, it is important to consider that standard responses to domestic violence safety planning are not effective for Indigenous communities (Gordon, Hallahan, & Henry, 2002).
Various studies recommend that a key feature for safety planning should include providing adequate safe houses and emergency shelters where individuals can feel secure (Bopp et al, 2003; Harper, 2011; Urbanski, 2001). However, at the same time there is a need for additional human and monetary resources within Indigenous communities to enhance such safety-planning measures (Dickson-Gilmore, 2014; NWAC, 2011). It is important to help women safety plan by teaching specific strategies, such as having ready both a packed bag and an escape route. This includes an emergency plan with the steps a woman will take when she recognizes she is in danger and arranging for a place where she can live in safety (Alberta Council of Women’s Shelter, 2014; Davis & Taylor, 2002).
The Native Women’s Association of Canada (2015) developed a toolkit to help Indigenous women experiencing various forms of discrimination and to assist women in recognizing their inner strength. Specifically, this toolkit emphasizes “Community Safety Planning” to categorize support systems and action plans to keep the woman and her children safe. It contains sections on what to do once she has left the relationship with information on social media safety, the Matrimonial Real Property Act, self-care, self-esteem, positive statements, healthy relationships, and survivor stories (NWAC, 2015).
Another toolkit, developed for Aboriginal families living off-reserve, is the MIYKIWAN toolkit (Congress of Aboriginal Peoples, 2015). This toolkit is framed around making Aboriginal traditions and teachings accessible while instructing families about various types of family violence, safety planning, and breaking the cycle of violence. Importantly, this toolkit seeks to bring awareness to families on a variety of violence-related issues including sexual violence, dating violence, violence against men, and violence against those with disabilities.
Additional recommendations for safety planning include developing comprehensive case plans that emphasize women’s strengths and capacities and also making sure that the victim and her children have a safe and stable home environment (Nixon et al., 2015; Thibodeau & Nixon, 2013; Muskoday Community Health Centre, 2012). In summary, important factors in safety planning are:
- limiting contact with the perpetrator of domestic violence to stabilize the family and allow for a safer home environment (Thibodeau & Nixon, 2013); and
- creating case plans that emphasize women’s strengths, capacities, and resources (Dickson-Gilmore, 2014; Nixon et al., 2015; Community Legal Information Association of Prince Edward Island, 2010).
Literature on domestic violence in Indigenous populations focuses mostly on risk assessment and identifies the need for further research on risk management and safety planning. Many research priorities have already been addressed in the above sections and are summarized below. Overall, it is imperative that future research on risk assessment, risk management, and safety planning consider the differences between and within Indigenous communities and cultures and also involve Indigenous peoples in their development, implementation, and evaluation.
Risk Assessment. There is a need for further research on risk assessment programs and tools that are culturally-located and -informed. As well, future research should focus on the evaluation of these tools and their impact in Indigenous communities. Recurrent recommendations include:
- developing a risk assessment instrument based on risk factors associated with violent offending in Indigenous communities (Allan & Dawson, 2002; Buchanan, 2009); and
- considering the geographic location of the victim in risk assessments as well as the multitude of unique risk factors associated with rural, remote, and northern location such as normalization of violence, lack of confidentiality and delayed medical response (Hampton et al., 2010; Davis & Taylor, 2002;(also see Literature review on Rural, Remote, and Northern hub).
Most risk assessments are based primarily on men’s history of abusive behaviour. Spiwak (2004) recommends that risk assessment should focus on females’ circumstances as well. For example, are they living in an isolated community? Do they have access to transportation or a phone? Do they have complicating factors such as a disability or an addiction? Understanding women’s circumstances will help to identify women most at-risk. When developing a risk assessment instrument for Indigenous women, it is recommended that predictors of risk of violence should be based on risk factors associated with violent offending in Indigenous communities (Allan & Dawson, 2002; Buchanan, 2009).
When assessing the risk of violence for Indigenous women, many prevalent factors are not included or considered. These factors include geographic isolation; the availability of firearms; the normalization of violence in a community; unemployment rate; quality of education; lack of mental health; social and policing services; overcrowding; and gender inequality (Davis & Taylor, 2002; Dreaddy, 2002; Shepherd, 2001; Brassard et al, 2015). Such factors contribute to higher rates of domestic violence in Indigenous communities and must be addressed.
When working with Indigenous communities on domestic violence and abuse, it is crucial to consider individual experiences with Indian Residential Schools. This involves being cognizant of Indigenous people’s historical and cultural background, including the process of colonization, and the loss of identity and traditional culture (Al-Yaman et al., 2006; Riel, 2013; Riel, Languedoc, Brown, & Gerrits, 2014). These factors increase Indigenous women’s risk of exposure to domestic violence.
Lastly, there is a need for Indigenous-led education on domestic violence for caregivers and support workers who work with Indigenous populations. This education would increase staff’s ability to recognize domestic violence, particularly among Indigenous children and youth. As well, more education is needed to help care for children and youth who may exhibit behaviour that is harmful to themselves and others. McKeown & Orr (2004) argue that allowing victims of violence to help educate society is an essential component of helping victims heal while also creating public awareness around the issue of domestic violence. Indigenous-led education will also help deconstruct the narrative of Indigenous women living high-risk lifestyles, which works to normalize domestic violence in families and communities (Assembly of First Nations, 2013).
Risk Management. Overall, mainstream approaches to risk management are considered culturally-inappropriate and ineffective and have led to the division of Indigenous families (Cripps, 2007). The inclusion and integration of spiritual ceremonies in domestic violence treatment has proven to be an effective strategy to manage risk in Indigenous populations (Puchala et al., 2010). Involving Indigenous staff in all aspects of offender programming ensures that interventions are culturally-appropriate and moves away from mainstream approaches. In offender treatment, cultural awareness training is useful in that it strengthens the cultural knowledge base of both Indigenous and non-Indigenous staff (Day et al., 2012).
Further research is required on the development and use of culturally-specific interventions and the role of both the family and the wider community in these interventions (Burnette et al., 2014). Managing risk must include an analysis of community processes to address power imbalances within Indigenous communities. Strategies should acknowledge the victims’ concerns while also involving members of the community (Cripps & McGlade, 2008). Using restorative justice initiatives in domestic violence cases facilitates community and Elders’ involvement. However, restorative justice is still a contentious topic among some researchers and advocates (Campbell, 2007).
Safety Planning. Research on safety planning should take a holistic approach and consider the many aspects of safety planning that are important in Indigenous communities (Bryant & Willis, 2008). The unique needs of Indigenous victims of domestic violence require further research. Currently, we know that safety plans should emphasize women’s strengths and capacities and involve Elders in the promotion of safety (Nixon et al., 2015; Riel et al., 2014b).
Research should look at the efficacy of limiting contact with the perpetrator and the victim and children. Some studies have found that limited contact is necessary to stabilize the family and to create a safer home environment (Thibodeau & Nixon, 2013). However, community dynamics can further complicate the ability to limit such contact. For example, some communities and/or families place greater importance on keeping the family together despite the increased risk for family violence. Furthermore, some communities silence discussion of domestic violence to preserve family and community cohesion (Brassard et al., 2015). Thus, considering what is best for the victim, perpetrator, children, and the wider community is a complex issue requiring further research.
Implications for Practice and Policy
Risk Assessment. Mainstream risk assessments do not fully capture the risk faced by Indigenous people. Since there is a link between the colonization of Aboriginal peoples and the impact of violence in these communities, risk assessments need to examine violence in the context of cultural continuity at individual and community levels (Brownridge, 2008).
The geographic location of the victim must be considered when developing or conducting a risk assessment. The overrepresentation of Indigenous populations in rural, remote, and northern areas presents a multiplicity of factors that must be considered. These include the community culture, lack of confidentiality, lack of social services, delayed police response, and delayed medical response (Hampton et al., 2010; Davis & Taylor, 2002; Dreaddy, 2002).
Health care centres, pediatric and adult healthcare, and mental healthcare providers should screen for abuse among all women, neither excluding nor targeting Indigenous women in particular. Further, it is imperative that resources exist for pediatric providers so that they can screen for abuse on a routine basis (Bohn, 2003).
Risk Management. Risk management practices should use holistic traditional practices such as addressing and treating (1) anger management, (b) loss of cultural identity, and (c) experiences of historical and current trauma and abuse (Amellal, 2005; Riggs, 2015). Overwhelmingly, research indicates that gaining knowledge from traditional knowledge holders, such as Elders and Healers, can be invaluable in the court system, health care system, and social services (Riel et al., 2014a; Blagg et al., 2015; Buchanan, 2009; Brown & Languedoc, 2004).
Some research indicates that domestic violence risk management should include reconnecting with Aboriginal tradition and spirituality. This can be done through spending time on the land, sharing and learning traditions such as storytelling, practices such as smudging and sweat lodge ceremonies, and providing guidance from spiritual Elders (Campbell, 2007; Lester-Smith, 2013; Thibodeau & Nixon, 2013).
While these recommendations appear to be applied generally, research maintains that culturally-relevant means of risk management should be specific to the community. Although few researchers discuss the specifics of community needs, it remains clear that needs differ between communities and that risk management strategies need to reflect these differences.
Safety Planning. Safety planning practices must work to empower Indigenous clients, many of whom have faced discrimination in the courts, within the health care and the social service systems, as well as in their daily lives (NWAC, 2015). Safety plans should recognize the impact of systemic discrimination, normalization of violence at home and in the community, and the impact of intergenerational trauma as a result of Indian Residential Schools. The involvement of Elders in the development of safety plans can assist in identifying the linkages between past abuse in Residential Schools and the intergenerational patterns of abuse that victims are coping with today. No single approach should be taken in safety planning with Indigenous populations, because the plan needs to be tailored to the specificity of the community.
Safety planning practices should consider factors that lie beyond the individual such as their formal and informal support networks, difficulties in accessing helping resources, and availability of culturally-appropriate responses (Gordon et al., 2002; Nixon et al., 2015). Culturally-appropriate practices should be implemented in safe houses, emergency shelters, and similar resources used by Indigenous clients.
There is a need for more human and monetary resources for social services, such as safe houses and emergency shelters, that provide safety plans to Indigenous people, particularly in rural, remote, and northern Indigenous communities (Bopp et al., 2003; Harper, 2011; Varcoe & Dick, 2008). Further, it is important to consider the differences between and within Indigenous communities in terms of a cultural safety model. Not all communities will have the same needs and not all communities will seek to address these needs in the same way. For instance, in communities that have adopted a Christian way of life, models which reflect the power of prayer and the church may be preferred.
Research on risk assessment, risk management, and safety planning with Indigenous peoples reveals several overarching themes:
- The history of colonization and subsequent intergenerational trauma from Indian Residential Schools presents complexities in the development, implementation, and evaluation of effective assessments, tools, and strategies.
- Mainstream approaches have been largely ineffective and can be harmful for Indigenous peoples and the communities in which they live.
- Practices should be culturally-appropriate, holistic, and consider the historical context of Indigenous peoples.
- Practices must be specific not only to the needs of individuals but also to the communities in which they reside.
- Overall, Indigenous-led and community-specific initiatives have been most effective in risk assessment, risk management, and safety planning.
- Therefore, Indigenous peoples must be involved in all stages of development, implementation, and evaluation of intervention strategies.
While there have been promising practices that place the unique needs of Indigenous peoples at the forefront of their design and implementation, much work remains to be done.
Rural, Remote, and Northern (RRN) populations
Authors: Anna Johnson, Danielle Bader, Nicole Jeffrey, Myrna Dawson
Contributors: Deborah Doherty, Melissa Wuerch, Diane Crocker, Wendy Verhoek-Oftedahl, Peter Jaffe, Jordan Fairbairn, Anna-Lee Straatman
Non-urban populations in Canada are at increased risk of domestic violence and homicide (Northcott, 2011; Statistics Canada, 2016a) and face several challenges (Bosch & Schumm, 2004; Maume, Lanier, Hossfeld, & Wehmann, 2014). Rates of domestic violence and domestic homicide in Canada are more than three times greater in rural areas than in urban areas (Northcott, 2011) and are highest in the Canadian territories (Bunge, 2002; Sinha, 2013; Statistics Canada, 2015). For example, the domestic violence rate is six times higher in Nunavut than Saskatchewan, the highest rate among the provinces (Statistics Canada, 2015). Furthermore, research indicates that the territories have the highest percentage of spousal violence incidents that involve physical force (Nunavut 77%; NWT 53%; Yukon 62%; Statistics Canada, 2008). While domestic violence perpetrator and victim characteristics in rural and urban environments are generally similar, research has indicated that (a) rural perpetrators may perpetrate more chronic and severe domestic violence (which could be associated with higher rates of substance abuse and unemployment); and (b) rural, remote, and northern (RRN) victims may have worse psychosocial and physical health outcomes due to the limited availability and accessibility of domestic violence services (Edwards, 2014; Logan, Walker, Cole, Ratliff, & Leukefeld, 2003; Peek-Asa et al., 2011).
Research indicates that RRN populations experience factors that may (a) increase vulnerability to domestic violence and homicide, (b) influence victimization experiences, (c) exacerbate victims’ negative mental and physical health outcomes, and (d) hinder victims’ ability and willingness to report abuse, obtain support and services, and leave an abusive partner. Table 2 reviews these factors. Given the increased risk of domestic violence and homicide as well as the many challenges faced by RRN populations, research on risk assessment, risk management, and safety planning among these populations is crucial. Nevertheless, most domestic violence research to date has been conducted in urban areas (see Beyer, Wallis, & Hamberger, 2015 for a review) and is not generalizable to RRN populations (Burke, O’Campo, & Peak, 2006).
Table 2: Rural, Remote, and Northern Population Vulnerabilities[6]
|
Risk Factor |
Examples |
|
Isolation |
Extreme weather; seasonal road conditions; long distances to services; limited access to personal and public transportation, Internet, telephone, and formal supports |
|
Economic and structural issues |
Higher cost of living; limited affordable/subsidized housing and employment opportunities; lower levels of income and education; community poverty |
|
Adherence to traditional and patriarchal religious and cultural values/norms |
Traditional family and gender-role views (e.g., man as head of household, DV as a private family matter), acceptance of abuse, and victim blaming attitudes/behaviours (including by counsellors and criminal justice providers, which can impede timely and effective responses) |
|
Barriers to service and support |
Limited availability or accessibility of services and other formal supports; slow emergency response time due to distance; lack of resources and proper training for domestic services, screening, and management |
|
Lack of privacy, anonymity, and confidentiality |
Dual relationships or familiarity with service providers, police, and law enforcement |
|
Strong traditions and community values around firearms |
Hunting and target practice traditions and more liberal gun safety views, which contribute to greater access to and use/threat of firearms in DV and homicide |
|
Farming |
Farming responsibilities, ownership of large farm animals, and generations of family farm ownership as barriers to leaving an abuser and/or seeking support. |
The paucity of domestic violence research (and clear conclusions based on research) within RRN areas may be due to the challenges associated with conducting and comparing research in these regions. For example, our review suggests that inconsistent and ambiguous definitions are used across research studies and that there are continued discussions around the best way of defining rurality. While most research understands “rural” broadly as a community or geographic location with a small and widely dispersed population distribution, definitions (when provided) vary based on degree of specificity (e.g., population size cut-off used or not), geographic level (e.g., county or sub-county), number of dimensions included (based on population size only or includes geographic, social, and cultural dimensions), theoretical framing (based on physical location or abstract system of understandings, values, and practices), and so on. Other definitions are ambiguous and only provide the location of the study. Currently, the CDHPIVP refers to the following working definitions based on several sources:
- Rural: A community or geographic location with a small and widely-dispersed population distribution (less than 10,000) (Statistics Canada, 2001)
- Remote: A community or geographic location that is not accessible by road year-round (Public Health Agency of Canada, 2009; Registered Nurses’ Association of Ontario, 2015)
- Northern: A community or geographic location that is designated by the provincial government as being the Northern part of the province (e.g., for Ontario, see http://nohfc.ca/en/about-us/northern-ontario-districts; for British Columbia, see www.northerndevelopment.bc.ca/about/northern-developments-region/) All the Canadian territories are considered northern.
This inconsistency creates difficulties when comparing results across studies and drawing conclusions about RRN domestic violence. Different definitions can also lead to different conclusions and policy implications (Hart, Larson, & Lishner, 2005). Nevertheless, the best definition may depend largely on the purpose for which it is being used or the research question being examined. For instance, while very specific definitions help to clearly classify rural and non-rural locations, they can be overly exclusionary in some cases. Some researchers have noted that the population standard of under 1,000 used by Statistics Canada (2016b) excludes many communities, because a population that low is rare in Canadian provinces such as Alberta (Zorn, Wuerch, Faller, & Hampton, 2017). While a unidimensional definition based solely on population size may offer a useful shorthand for identifying populations of interest, a multidimensional definition may help to better identify the characteristics of rurality that are particularly important in the experience of domestic violence (e.g., a community with a population of 1000 but is 10km away from a city with a population of 100,000 where services can be accessed).
Additional challenges associated with conducting research in RRN regions include:
- difficulty accessing RRN populations due to geographic and social isolation (Moffitt et al., 2013);
- sample size and participant confidentiality issues due to smaller populations (Rural Health Information Hub, 2016);
- a “cloak of silence” that supports the belief that domestic violence is a private matter (Doherty & Hornosty, 2004);
- difficulty generalizing or transferring research findings across diverse RRN regions (Rural Health Information Hub, 2016); and
- limited risk assessment, risk management, and safety planning tools specific to RRN populations.
Due in part to these challenges, efforts to understand and combat domestic violence and homicide among RRN populations are in their early stages. In the following sections, we review the limited research that has examined domestic violence risk assessment, risk management, and safety planning among RRN populations. One important note is that much of the research within the literature review has a greater focus on ”rural” communities and less of a focus on ”remote” and/or “northern” (i.e., Anderson, Renner, & Bloom, 2014; Annan, 2008; Averill, Padilla, & Clements, 2007; Banman, 2015; Bender, 2015; Beyer et al., 2013; Bhandari, Bullock, & Sharps, 2013; Biesenthal et al., 2000; Bloom et al., 2014; Bosch & Bergen, 2006; Bosch & Schumm, 2004; Choo, Newgard, Lowe, Hall & McConnell, 2011; Davis, Taylor, & Furniss, 2001; Doherty & Hornosty, 2008; Dudgeon & Evanson, 2014; Eastman & Bunch, 2007; Eastman et al., 2007; Edwards, 2014; Edwards et al., 2014; Evanson, 2006; Fitzsimons, Hagemeister, & Braun, 2011; Gadomski, Tripp, Wolff, Lewis, & Jenkins, 2001; Grama, 2000; Grossman et al., 2005; Hassija & Gray, 2011; Hornosty & Doherty, 2002; Jamieson & Wendt, 2008; Kasdorff & Erb, 2010; Krishan, Hilbert, & Pase, 2001; Lanier & Maume, 2009; Logan et al, 2003; Maume et al, 2014; McCall-Hosenfeld et al., 2014; Owen & Carrington, 2015; Peek-Asa et al., 2011; Potts, 2011; Ragusa, 2012; Rennison, DeKeseredy, & Dragiewicz, 2013; Revuelto, 2002; Riddell, Ford-Gibloe, & Leipert, 2009; Sandberg, 2013; Stokes, 2012; Ulbrich & Stockdale, 2002; Van Hightower & Gorton, 2002; Wendt & Hornosty, 2010; Wisniewski, Arseneault, & Paquet, 2016; Wolf, 2015).
Key Findings in Risk Assessment with RRN Communities
Most of the RRN domestic violence risk research to date has focused on factors that may increase RRN women’s vulnerabilities to domestic violence (see Table X above). Research comparing RRN and urban risk factors for domestic violence has found that perpetrator and victim characteristics in rural and urban/suburban environments are generally similar (see Edwards, 2014 for a review). The very limited research that has empirically compared RRN and urban risk factors for domestic homicide has found important demographic, psychological, and situational differences. For example, research has found that partners were significantly less likely to be separated (Banman, 2015) and significantly more likely to be married in rural compared to urban cases of domestic homicide (Beyer, Layde, Hamberger, & Laud, 2013). This may be related to the adherence to traditional family values and cultural norms as well as the barriers to leaving an abusive partner (e.g., isolation, lack of resources, or community values) that exist in rural communities (Banman, 2015; Doherty & Hornosty, 2008). Rural perpetrators were significantly less likely to exhibit obsessive behaviour and sexual jealousy (based on the Domestic Violence Death Review Committee database and individual case reports), perhaps because of lower levels of separation which might lead men to attempt to regain control (Banman, 2015). Rural victims were significantly less likely to live in neighbourhoods characterized by residential instability (i.e., proportion of individuals living in a different house than they had 5 years before; Beyer et al., 2013). This suggests that the common usage of residential instability to indicate disrupted social cohesion and violence risk may not apply to rural settings. Instead, residential stability might indicate social relationships marked by lack of privacy, anonymity, and feeling trapped.
Finally, research has highlighted the role of gun culture in RRN communities. Firearms play an important role in RRN culture, which includes strong traditions around hunting, target practice, and other law-abiding activities, as well as more liberal gun safety views (Banman, 2015; Doherty & Hornosty, 2008). However, these firearms often become weapons of fear, control, and violence within families experiencing domestic violence (Banman, 2015; Doherty, 2006; Doherty & Hornosty, 2008). A review of domestic homicide cases in Ontario between 2003 and 2012 (using the Domestic Violence Death Review Committee database) found that rural[7] perpetrators were significantly more likely than urban perpetrators to have access to a firearm (51.5% versus 23.9%) and to use a firearm to kill their partner (45.5% versus 17.5%; Banman, 2015). Rural perpetrators were also significantly more likely to use a gun (46%) to kill their partner compared to a knife (21.2%) or any other weapon (33.3%; Banman, 2015).
Risk assessment tools. This literature review did not identify any risk assessment tools specific to RRN populations. The review highlighted that using generic tools may not capture the specific risks associated with these populations. Some research recommends that in addition to standard or generic risk assessment questions, risk assessment tools should ask questions that assess the different risks for RRN women including (a) distance from closest neighbour, (b) access to a telephone, transportation, and social support, (c) awareness of and willingness to use nearby services, (d) perpetrator misuse and abuse of firearms, and (e) perpetrator abuse towards pets and farm animals (Doherty & Hornosty, 2008; Dudgeon & Evanson, 2014).
Role of community professionals. RRN healthcare settings—such as family planning clinics, emergency departments, and county health departments—have been identified in the literature as important points of intervention for universal screening (Anderson et al., 2014; Guimei, Fikry, & Esheiba, 2012; McCall-Hosenfeld et al., 2014; Neill & Hammatt, 2015; Ulbrich & Stockdale, 2002; Van Dyke, 2005). This is because RRN jurisdictions often have fewer specialized services for domestic violence than urban settings and RRN women tend to have more frequent contact with health care providers compared to other formal service providers (Bhandari et al., 2013; McCall-Hosenfeld et al., 2014). This screening may occur regularly to detect the history and seriousness of domestic violence as well as the victim’s ability and readiness to take protective action (Dudgeon & Evanson, 2014; Neill & Hammatt, 2015; McCall-Hosenfeld et al., 2014; Van Hightower, Gorton, & DeMoss, 2000). Nevertheless, this universal screening in RRN healthcare settings is not yet standard practice (Choo et al., 2011; McCall-Hosenfeld et al., 2014). Research suggests that a smaller proportion of rural healthcare providers and emergency departments have official domestic violence screening policies and standardized screening instruments compared to urban areas due to barriers such as competing priorities, limited resources, and insufficient training (Choo et al., 2011; McCall-Hosenfeld et al., 2014). Furthermore, screening for DV in healthcare settings is a debated issue in the field (Wathen & MacMillan, 2013; MacMillan et al, 2009). There are concerns about possible adverse effects of DV screening such as psychological distress, family disruption, reprisal violence, and children being removed from the home after DV is identified (MacMillan et al., 2009). There is also concern that healthcare providers are not adequately trained to know how to respond to DV and that universal DV screening is ineffective in the absence of interventions and resources required to support women identified by the screening tool (Choo et al., 2011; MacMillan et al, 2009; McCall-Hosenfeld et al., 2014).
Role of technology. Given the vulnerabilities and barriers for RRN populations related to physical and social isolation (e.g., limited access to transportation), limited availability of services, and privacy concerns, web- and computer-based risk assessment tools have the potential to increase accessibility to risk assessment and safety planning strategies for RRN victims (Bloom et al., 2014). For example, several safety decision aids exist to guide women through risk assessment, to help them consider safety-related priorities (e.g., child’s wellbeing, having resources, maintaining privacy, or feelings for partner) and to develop tailored safety plans (Bloom et al., 2014). These cost-effective tools can be used in diverse settings, including healthcare settings, welfare offices, community agencies, libraries, and women’s own homes when safe and convenient (Bloom et al., 2014; Glass et al., 2010). However, many of these aids rely on access to the internet, and there may be no connectivity in rural, remote, and northern areas of the country.
Research testing web- and computer-based risk assessment tools among RRN populations remains limited. For example, Bloom et al. (2014) evaluated the feasibility of a web-based risk assessment and safety planning tool specifically for pregnant women experiencing domestic violence in urban and rural communities. They found that a greater proportion of women in rural jurisdictions accessed the tool from a home computer compared to women residing in urban jurisdictions. No adverse events related to the study were reported, providing some possible evidence for the safety of the web-based tool.
Key Findings in Risk Management with RRN Communities
Much of the literature to-date on reducing domestic violence and homicide among RRN populations discusses the need for broad community prevention efforts and sociocultural shifts rather than specific strategies intended to reduce risk among individual perpetrators (i.e., risk management as defined by the CDHPIVP). This literature suggests:
- focusing on increasing access to housing, transportation, financial security, parenting/childcare support, and culturally-appropriate resources (e.g., healing circles; Barton, Hungler, McBride, Letourneau, & Mailloux, 2015; Hornosty & Doherty, 2002); and
- shifting cultural norms that support beliefs in traditional gender roles and patriarchy and increasing knowledge about domestic violence and healthy relationships (e.g., through educational programs and public health campaigns; Barton et al., 2015; Gadomski et al., 2001; Jamieson & Wendt, 2008; Van Dyke, 2005).
Limited research has tested such efforts. However, one study evaluated a public health campaign implemented in 10 rural counties in central New York and that involved radio advertisements, posters, mailings to libraries and clergy, distribution of media articles and printed advertisements, as well as health facility modifications (e.g. modifications to emergency department records, victim rights statement, safety planning brochure, or list of domestic violence services; Gadomski et al., 2001). The findings revealed statistically-significant increases in the intervention counties in relation to slogan and advertising recognition, particularly among men. Both men and women in the intervention counties reported believing that residents of the community would talk to a victim, consult with friends, or talk to a doctor if they knew a neighbour next door was abusing his partner. However, this finding was more significant among men with an increase of 13% post-campaign compared to an increase of 4% for women. Additionally, men who heard the slogan “no one deserves to be abused” increased by 18% post-campaign, while there was no change among women pre- to post-campaign with slogan recognition. Overall, calls to the domestic violence agency hotline in the intervention community doubled after the conclusion of the campaign (Gadomski et al., 2001), thus concluding that public education campaigns may be particularly valuable for reaching men in rural communities.
The limited literature that has examined specific risk management strategies for RRN perpetrators recommends implementing:
- firearm confiscation, removal, and restricted access policies for those with a history of domestic violence or those subject to a protection order (Banman, 2015; Doherty, 2006; Doherty & Hornosty, 2008);
- “safe at home” program models whereby the perpetrator is removed from the family home, allowing women and children to remain in the home when safe (Social Development Committee of the Parliament of South Australia, 2016); and
- more meaningful consequences for perpetrating domestic violence in the justice and court system, such as increased prosecution by county attorneys (Barton et al., 2015; Revuelto, 2002).
Generally, research suggests that the criminal justice response to domestic violence in RRN communities may be inadequate. Currently, perpetrators are treated leniently (especially if they are respected members of the community; Fitzsimons et al., 2011; Van Hightower & Gorton, 2002), and victims experience difficulties in obtaining and enforcing protection orders (Dudgeon & Evanson, 2014; Fitzsimons et al., 2011). Interviews with victims/survivors living in rural Texas reported discourteous and victim-blaming interactions with criminal justice personnel (Van Hightower & Gorton, 2002). These patterns are likely a product of the patriarchal norms (e.g., victim blaming or DV seen as a private rather than a criminal matter), dual relationships, and lack of training (as noted above) that exist in many RRN communities (Van Hightower & Gorton, 2002). Moreover, although the criminal justice system relies heavily on protection orders as a risk management strategy, research suggests that victims in RRN communities experience barriers such as fees and lack of confidentiality, to obtaining and enforcing protection orders (Dudgeon & Evanson, 2014; Fitzsimons et al., 2011; Wider Opportunities for Women, 2013).
Key Findings in Safety Planning with RRN Communities
Much of the domestic violence literature on safety among RRN populations has examined the strategies that RRN victims employ to protect themselves and their children. Findings suggest that resistance and placating strategies[8] are most common. These include leaving the home, ending or trying to end the relationship, fighting back physically or verbally, trying to avoid an argument with the abuser, and doing whatever the abuser wants to stop the violence (Anderson et al., 2014; Riddell et al., 2009). While the protective strategies used by RRN women are similar to those used by urban women, RRN women appear to rely more heavily on informal supports, such as family, friends, and community members, likely because of the limited availability and accessibility of formal supports and (emergency) services (Nixon et al., 2015). Even when formal services are available to RRN women, social, cultural, and practical barriers often still prevent women from accessing them; these barriers include isolation, traditional patriarchal values, and others noted in Table X (Riddell et al., 2009). Moreover, while resistance and placating strategies are most common, they are noted as among the least helpful (Anderson et al., 2014; Riddell et al., 2009). RRN women, instead, report that strategies such as developing an escape plan, developing a code so that others know she is in danger, hiding important papers from the abuser, staying in a shelter, and sending children to stay with family or friends are more helpful (Anderson et al., 2014; Riddell et al., 2009).
Given the vulnerabilities experienced by RRN victims (see Table 2), safety planning in these communities requires additional considerations and should include the complexity of each woman’s circumstances (Barton et al., 2015). For example, RRN women often face additional barriers to leaving an abusive partner, including: (a) long-established ties to family, the community, and property (e.g., farm property that has been in the family for generations); (b) traditional values toward keeping the family together; and (c) economic dependence on the abuser and/or lack of employment opportunities; and farming responsibilities (Doherty & Hornosty, 2004; Social Development Committee of the Parliament of South Australia, 2016). Because leaving an abusive relationship is not always a viable option among RRN victims, safety planning should be done with sensitivity and an understanding of the rural context with a focus on plans to minimize potential harm to women rather than encouraging them to end the relationship (Doherty & Hornosty, 2004).
The limited availability and awareness of domestic violence services in many RRN communities suggest that service providers need to work more with women to identify both formal and informal supports (Bosch & Bergen, 2006; Dudgeon & Evanson, 2014; Edwards, 2014). Further, creative solutions may need to be brainstormed in cases where shelters and safe houses are limited or inaccessible (e.g., identifying a safe hiding place in a victim’s barn; Evanson, 2006). Many pet-owning RRN victims report that their abusive partners have threatened or harmed their pets and that concern for their pets has affected their decisions to stay or leave an abusive partner (Faver & Strand, 2003). Though findings are similar for pet-owning urban victims, women in RRN areas are more likely to have larger farm animals and are less likely to have access to shelters and other services. Therefore, safety planning in these areas should include arrangements for pets (e.g., “safe haven” programs; Faver & Strand, 2003). Finally, safety planning efforts should address confidentiality concerns faced by many RRN people to help women feel comfortable disclosing experiences of abuse to health care and other service providers (Bender, 2015).
Role of technology. As with risk assessment, web- and computer-based tools may play an important role in safety planning among RRN domestic violence victims. For example, web- and computer-based safety decision aids can be used to guide women through risk assessment and safety priority setting (i.e., rating the importance of child’s wellbeing, concern for safety, having resources, preserving privacy, and feelings for partner) and to develop tailored safety plans (as described above; Bloom et al., 2014). Some of these tools (e.g., Bloom et al., 2014) are designed to provide women from nonmetropolitan residences with additional RRN-specific strategies on their tailored safety plans. Videoconferencing can similarly be used to provide trauma-focused treatment and other services depending on internet connectivity (e.g., using Skype or Facetime to attend court when women cannot easily leave their homes; Barton et al., 2015; Hassija & Gray, 2011). Other technologies that can support safety planning among RRN victims include GPS technology (e.g., “Safe Tracks”) to respond quickly to domestic violence incidents by locating women instantly (Barton et al., 2015) and toll-free crisis hotlines (Hornosty & Doherty, 2002). In addition to reducing accessibility barriers for victims, such technologies can also help to connect isolated and distant collaborators and stakeholders in service development and to support training delivery to RRN areas (Neill & Hammatt, 2015).
Role of informal supports. Despite RRN women’s heavy reliance on and perceived helpfulness of family, friends, and community members (Nixon et al., 2015; Riddell et al., 2009), such informal supports may not always be effective at keeping women safe from abuse. For example, Bosch and Schumm (2004) found that access to resources (pertaining to safety, telephone/computer access, transportation, informal network, formal network, housing availability, and money/job opportunities) is important for reducing abuse among RRN women and that having supportive persons predicted declines in abuse only when that support helped women access resources. Thus, research suggests that emotional support is not enough for keeping RRN women safe; informal supports should also offer information and advice to help victims access resources. Moreover, RRN women’s informal networks often offer conflicting advice, blame the victim, ignore the abuse, and/or hinder access to resources; all of this can heighten women’s stress and keep them bound in abusive relationships (Bhandari et al., 2013; Bosch & Schumm, 2004). Bosch and Schumm (2004) suggest that, anecdotally, RRN women sometimes wish that their support network had been more persistent in maintaining communication and asking questions about the abuse, especially when they had limited outside contact (e.g., no telephone, telephone usage monitored/restricted, or not able to visit others).
Role of community professionals. Safety plans are predominantly developed with victims by social service providers (e.g., social workers and counsellors); however, some researchers suggest that those in healthcare settings (e.g., Primary Care Physicians, [Forensic] Nurses, or practitioners in family planning clinics) can also help develop safety plans, especially in RRN areas (Anderson et al., 2014; Laughon, Sutherland, & Parker, 2011; McCall-Hosenfeld et al., 2014; Neill & Hammatt, 2015; Ulbrich & Stockdale, 2002). Nurses are especially well-positioned to support domestic violence victims and, as some researchers suggest, should be knowledgeable about the needs and experiences of RRN women to provide care that addresses their needs (Dudgeon & Evanson, 2014; Neill & Hammatt, 2015). Because RRN women often access healthcare settings outside of their communities, it is suggested that urban nurses should also be trained in supporting RRN women (Neill & Hammatt, 2015).
Farm organizations (e.g., Dairy Farmers of New Brunswick, Farm Animal Council of Saskatchewan, Provincial Federations of Agriculture, Canadian Federation of Agriculture, Canadian Agricultural Safety Association, Christian Farmers Federation of Ontario, National Farmers Union, Rural Ontario Institute, and Canadian Agricultural Human Resource Council www.agriguide.ca) have also been identified as an important point of contact between victims and domestic violence service providers in RRN communities (Kasdorff & Erb, 2010). Given their important role in many RRN communities, these organizations might be able to share a list of available services with victims and help DV service providers to identify RRN concerns and ways to address them (Kasdorff & Erb, 2010).
Efforts to understand and to combat domestic violence and homicide among RRN populations are in their early stages. More work is still needed in the areas of research, policy, and practice to better understand and meet the needs of RRN communities (Annan, 2008; Neill & Hammatt, 2015; Owen & Carrington, 2015; Sandberg, 2013). This section highlights the current gaps in the RRN domestic violence literature and recommendations for future research. In addition to the general scarcity of domestic violence research among RRN populations noted above, there are also several gaps in research that has examined RRN populations. For example, researchers have highlighted the need for:
- qualitative and methodologically rigorous studies (Annan, 2008);
- research that extends beyond the individual and relational correlates of domestic violence and examines community context (Edwards, Mattingly, Dixon, & Banyard, 2014);
- research among RRN men to better understand risk factors and why they abuse (Rennison et al., 2013);
- research on the co-occurrence of other issues, such as substance abuse, and DV in RRN settings (Logan, Walker, & Leukefeld, 2001);
- research on the challenges and vulnerabilities faced by RRN women, especially research which empirically compares these vulnerabilities with other environments (Dawson, Hubbert, & Poon, 2010; Edwards, 2014); and
- research among diverse RRN populations, including RRN women of colour, RRN women with disabilities, Indigenous populations living in RRN areas.
Implications for Practice and Policy
Several recommendations for practice have been made across risk assessment, risk management, and safety planning literature to address some of the barriers and vulnerabilities noted in Table 2. These include increased training for service providers, increased services, and addressing RRN accessibility barriers. First, many have noted the importance of increased training and education for RRN service providers about domestic violence, with a focus on how social and cultural contexts specifically impact RRN women (Barton et al., 2015; Jamieson & Wendt, 2008; Neill & Hammatt, 2015; Riddell et al., 2009; Wendt & Hornosty, 2010). This training and education is critical for those who conduct risk assessment, risk management, and safety planning (including those in the healthcare setting), for those who respond to disclosures of abuse, and for criminal justice personnel (Krishnan et al., 2001; McCall-Hosenfeld et al., 2014; Neill & Hammatt, 2015; Ragusa, 2012). Second, many have stressed the need for both developing and implementing more and new services for perpetrators and victims and also increasing funding and resources for such services to address current scarcity in many RRN communities (Anderson et al., 2014; Barton et al., 2015; Logan et al., 2001; Neill & Hammatt, 2015; Riddell et al., 2009; Wendt & Hornosty, 2010).
Finally, given the physical and social isolation and limited availability of services in RRN communities, strategies have been recommended for reducing barriers and increasing access to risk management and safety planning services, such as increasing availability of services beyond weekdays and beyond 9:00am to 5:00pm (Barton et al., 2015) and including domestic violence interventions in pre-existing rural substance abuse treatment programs (Logan et al., 2001). Service providers might also help to reduce transportation and geographical barriers by (a) providing transportation support (especially for programs that are outside RRN communities); (b) using volunteers to transport victims to domestic violence service providers; and (c) implementing outreach services so that existing urban services and advocacy organizations can travel to RRN areas (Campo & Tayton, 2015; Grama, 2000; Greenard-Smith, 2003; Hornosty, Doherty, 2002; Jamieson & Wendt, 2008; Logan et al., 2003; Neill & Hammatt, 2015).
Service collaboration and coordination. Multisector communication and collaboration and coordinated community responses may play an important role in addressing RRN domestic violence (Eastman, Bunch, Williams, & Carawan, 2007; Gallup-Black, 2004; Potts, 2011). For example, police, probation, healthcare, housing, and other social services might collaborate by sharing information, assessing cases, and agreeing on an action plan (Potts, 2011). Similarly, implementing integrated case management (i.e., various service providers meet regularly to discuss current cases, to review how clients are progressing, and to offer coordinated services) has been recommended for domestic violence risk management and safety planning in RRN communities (Barton et al., 2015; Gallup-Black, 2004; Neill & Hammatt, 2015). Such efforts can reduce transportation barriers for victims and perpetrators, facilitate holistic care for families affected by domestic violence by attending to the needs of the whole family, and improve monitoring and identification of high-risk victims and perpetrators in RRN jurisdictions (Hornosty & Doherty, 2002; Potts, 2011). Similarly, comprehensive “wrap around” services for women that include shelter services, support accessing housing and transportation, economic assistance, childcare support, access to mental health services and therapists, and education funding to provide long-term, self-sustaining employment possibilities may be useful (Barton et al., 2015).
Immigrant and Refugee Populations
Authors: Sarah Yercich, Kate Rossiter
Contributors: Abir Al Jamal, Randal David, Mohammed Baobaid, Margaret Jackson
Understanding the elevated and specific risks for domestic violence and homicide within immigrant and refugee populations is predicated on the grounds of complex, often intersecting vulnerabilities that are closely linked to cultural, religious, and gender ideologies as well as experiences of migration, acculturation (i.e., adaptation following contact between people of different cultures), and marginalization (Rees & Pease, 2007). Being caught between two cultures (i.e., home and host countries), immigrant and refugee women are in unique and distinctively vulnerable positions during and post-migration (for example, see Baobaid, 2012).
By comparison with their non-immigrant/refugee counterparts and as a collective population, these groups are more vulnerable and are at an elevated risk for domestic violence, which results from compounding and interrelated individual, familial, cultural, social, and systemic level risk factors (Amanor-Boadu, 2009; Amanor-Boadu, Messing, Stith, Anderson, O’Sullivan, & Campbell, 2012; Frye, Galea, Tracy, Buccialrelli, Putnam, & Wilt, 2008; Hassan, Thombs, Rousseau, Kirmayer, Feightner, Ueffing, & Pottie, 2011; Rothman, Gupta, Pavlos, Dang, & Coutinho, 2007). Grouping these vulnerable populations into a single category, however, fosters the homogenization of immigrant and refugee experiences (Burnman, Smailes, & Chantier, 2004; Raj & Silverman, 2002). Assumptions of uniformity in experiences not only heightens the risks faced by these women but also creates barriers to help-seeking and service provision.
Victims/survivors of violence within immigrant and refugee populations share some common challenges, barriers, and risks linked to legal status, language, culture, and lack of familiarity with Canadian systems. However, many experiences and vulnerabilities present differently within the wide variety of immigrant and refugee populations residing in Canada. These differences are exemplified through unique risk factors, manifestations of violence, and barriers to help-seeking (Raj & Silverman, 2002). For example, the vulnerabilities and risks experienced by immigrant and refugee women from Middle Eastern cultures, which are rooted in collectivism (i.e., prioritizing the group and family over the individual), differ from the vulnerabilities inherent in East Asian culture, which is based in Confucian traditions of social harmony (i.e., reduction of social and class conflicts) (Lee, 2000).
Understanding domestic violence and homicide in immigrant and refugee populations requires a lens that considers the contexts of migration, culture (e.g., individualism or collectivism), and diverse values and beliefs[9]. Further, domestic violence and related homicides may also be linked to other forms of gender-based violence including honour- and dowry-related crimes and child- and forced-marriages, though these crimes are not necessarily linked to culture. In order to understand domestic violence and homicide in immigrant and refugee populations and to address risk and safety issues, a broader, culturally-informed lens is critical (Lee & Hadeed, 2009).
Key Findings for Risk Assessment with Immigrant and Refugee Populations
Risk assessment involves evaluating the level of risk of harm to a victim/survivor; this includes risk of repeated violence and lethal violence. For immigrant and refugee populations, risk for domestic violence perpetration and victimization varies based on immigration status, length of stay in host country, and culture (Bauer, Rodriguez, Quiroga, & Flores-Ortiz, 2000; Hassan et al., 2011; Hyman & Forte, 2006), as well as migration processes, acculturation levels, gender role expectations, socioeconomic status, marginalization, religious beliefs, and socio-cultural influences (e.g., cultures that highly value family honour) (Ben-Porat, 2010; Celaya-Alston, 2010; Klevens, 2007; Muhammad, 2010; Sokoloff, 2005).
While some risk factors may be common among immigrant and refugee populations, it is also important to recognize the heterogeneity of immigrant and refugee populations to identify unique risk factors within different cultural groups. Research on the dynamics of domestic violence among immigrant and refugee populations has identified some important differences between groups from diverse cultural backgrounds. In cultures where traditionalism and conservatism are valued, and where patriarchal values lead to strictly defined gender roles (i.e. men having significantly more power than women), domestic violence may be more pervasive. For example, research with immigrants and refugees, including Vietnamese (Taft, Small, & Hoang, 2008), Chinese (Jin & Kent, 2010; Lee, 2000; Yick & Ooman, 2009), Japanese (Yoshihama, 2001), Indian (Natarajan, 2002), and Confucian-based (Sabri, Campbell, & Dabby, 2015) populations, finds that traditional patriarchal values and hierarchical gender structures create tolerance for domestic violence (Korteweg, 2012; Liao, 2006).
Immigrant and refugee women face increased vulnerability and risk due to geographic and social isolation, language barriers, cultural norms that perpetuate silence around domestic violence, traditional gender roles, economic dependence, normalization of violence, lack of information about laws and available support services, and discrimination (for example, see Choi, 2015). Women who immigrate illegally may not have identification documents, particularly if their abusers confiscate these documents and control their partners’ finances (Moynihan, Gaboury, & Onken, 2008). Women in these situations are more likely to be subjected to control tactics that involve threats of deportation (Erez et al., 2009). Accordingly, risk assessments should be conducted using comprehensive, objective, validated, and consistent tools that also consider the specific cultural contexts and circumstances of immigrant and refugee survivors (Light et al., 2008).
Community and cultural norms may influence the awareness of (and thus assessment of) domestic violence risk. For example, help-seeking behaviours are hindered for many immigrant and refugee survivors because of the “stigma, sensitivity, and silence” surrounding domestic violence; this is reflected in research with both Tamil communities (Hyman, Mason, Guruge, Berman, Kanagaratnam, & Manuel, 2011, p. 782) and Somali women, for whom violence and mental health concerns have been associated with weakness (Nilsson, Brown, Russell, & Khamphakdy-Brown, 2008). Further, some women from Korea and other Asian countries may risk humiliation, stigma, and shame if they disclose experiences of domestic violence (Lee, 2007; Midlarsky, Venkataramani-Kothari, & Plante, 2006). As such, domestic violence often remains hidden in collectivist cultures (Jin & Kent, 2010; Lee, 2000; Natarajan, 2002; Yick & Ooman, 2009) where concepts of family unity, honour, and shame are important (Belfrage, Strand, Ekman, & Hasselborg, 2012a; Kulwicki, Aswad, Carmona, & Ballout, 2010; Shalabi, Mitchell, & Andersson, 2015).
Women survivors among immigrants and refugees from Latin American countries may suffer domestic violence for longer periods or may stay in abusive relationships for longer durations, as a result of core cultural values such as ‘familismo’ (i.e., critical role or importance of immediate and extended family ties) (Acevedo, 2000; Brabeck & Guzmán, 2009; Dutton, Orloff, & Aguilar Hass, 2000; Fuchsel, Murphy, & Dufresne, 2012; Kyriakakis, 2014; Lewis, West, Bautista, Greenberg, & Done-Perez, 2005; Silva-Martinez, 2016). Cultural factors, such as “cultural permissiveness toward drinking, or socialization either to drink or abstain from alcohol consumption” (Lee & Hadeed, 2009, p. 156) can also serve as risk or protective factors with respect to domestic violence (see also Chung, 2006).
Risk Factors. The risk factors experienced by abused immigrant and refugee women in Canada include: (a) experiences and stressors of migration and acculturation (for example, see Ben-Porat, 2010; Brownridge & Hall, 2002; Hazen & Soriano, 2005; Hyman, Forte, Mont, Romans, & Cohen, 2006; Liao, 2006; Natarajan, 2002; Nilsson et al., 2008; Novick, Yoshihama, Runner, & Fund, 2009; Rees & Pease, 2007); (b) culturally-embedded and gendered roles and expectations, which are often challenged within the western context (for example, see Ben-Porat, 2010; Huerta, 2014; Kim & Sung, 2016; Muhammad, 2010); (c) patriarchal and religious ideologies rooted in male dominance and family unity (for example, see Lee, 2007; Muhammad, 2010; West, 2015); (d) lack of English language proficiency (for example, see Fong, 2000; Kim & Sung, 2016; Novick et al., 2009; Shalabi et al., 2015; Shiu-Thornton, Senturia, & Sullivan, 2005; Trijbetz, 2011; Vives-Cases, Torrubiano-Dominguez, Gil-Gonzalez, La Parra, Agudelo-Suarez, Davo, & Martinez-Roman, 2014); (e) poverty, un/under employment, and low socioeconomic status post-migration, as well as financial dependence (for example, see Ben-Porat, 2010; Kim & Sung, 2016; Muhammad, 2010; Novick et al., 2009; Vidales, 2010; West, 2015); (f) precarious or no legal status, as well as power dynamics and legal barriers related to sponsorship (for example, see Hancock & Siu, 2009; Huerta, 2014; Kim & Sung, 2016; Novick et al., 2009; Vives-Cases et al., 2014); (g) social, cultural, and economic isolation (for example, see Fong, 2000; Hyman et al., 2011; Keller & Brennan, 2007; Muhammad, 2010; Novick et al., 2009; Trijbetz, 2011); (h) lack of knowledge of Canadian systems/laws/culture (for example, see Fong, 2000; Novick et al., 2009; Pendleton, 2003; Rothman et al., 2007; Vaughan et al., 2015); (i) culturally-embedded beliefs that are supportive of and conducive to intimate partner violence (Klevens, 2007); and (j) shifts in family dynamics post-migration (Welland & Ribner, 2010). Vulnerabilities and risks such as these are further intensified by culture clash, lack of cultural competency among service providers, racism at the systems’ level (for example, see Edelstein, 2013), and fear of stigma or exclusion at the community level (for example, see Trijbetz, 2011).
These risk factors heighten barriers between migrant populations and supports within Canadian society, which further compromises the safety of immigrant and refugee women. Within these populations, male perpetrators also present unique risk profiles such as embedded beliefs in patriarchal authority, unbalanced gender roles, resistance to Westernization, and weakened cultural norms post-migration (for example, see Welland & Ribner, 2010). In addition to the unique risk factors and increasingly complex vulnerabilities, the manifestations of abuse within these populations are distinct in that some forms of violence are based in non-Western ideologies, such as so-called honour violence and/or killings (for example, see Baobaid & Hamed, 2010; MOSAIC, 2015). These risks and dynamics of domestic abuse in immigrant and refugee populations increase the likelihood for both repeated and escalating violence.
Risk Assessment Tools: Culturally-Informed and Multidimensional Risk Assessment. Among immigrant and refugee populations, risk for severe, escalating, and potentially lethal domestic violence increases at later stages of the migration and settlement processes (i.e., after the initial integration into the receiving society) due to factors such as acculturation and the experience of cultural conflict (Du Mont, Hyman, O’Brien, White, Odette, & Tyysa, 2012; Hyman et al., 2006). As such, assessing the risk related to domestic violence and homicide in immigrant and refugee populations is most effective when using both culturally-informed (for example, see Hyman & Forte, 2006) and multidimensional (Lee, 2007) perspectives. For example, through an analysis of the factors that increase risk for severe domestic violence in Korean immigrant populations, Lee (2007) emphasizes that identifying key ethno-cultural and sociocultural aspects of risk, along with standardized, validated risk assessment tools (or instruments), is fundamental to effective interventions with diverse ethno-cultural communities.
A multidimensional risk assessment model also includes consideration of help-seeking trends within immigrant and refugee communities to provide a holistic understanding of factors that influence access to, and use of, formal (e.g., health, justice, or anti-violence) and informal supports (Lee, 2007; Sharma, 2007). This approach reflects Hamby’s (2008) holistic risk assessment approach that accounts for financial, social, and legal risk factors in addition to assessments of risk to self and others (as cited in Amanor-Boadu, 2009; see also Amanor-Boadu, et al., 2012).
Although a review of the domestic violence literature reveals few culturally-specific risk assessment tools, some of these tools are noteworthy. For example, the PATRIARCH tool aims to assess risk for so-called honour-based violence (Belfrage et al., 2012a). Belfrage et al. (2012a) explore how law enforcement and service providers manage risk after conducting the PATRIARCH and also suggest that further research is needed to explore additional risk factors that might not be captured in this tool. Of note, Baobaid (n.d.) recommends the use of the Four Aspects Screening Tool (FAST) when working with minority families, as this tool addresses four domains that function as sources of risk within minority and immigrant communities: (1) universal, (2) ethno-cultural, (3) migration, and (4) religious. Similarly, Chan (2012) contends that the Chinese Risk Assessment Tool for Victims (CRAT-V) has “several advantages for the prediction of intimate partner violence in the Chinese population” (p. 161) because it accounts for culture- and population-specific risks in addition to variables that have an impact on disclosure and reporting of domestic violence within this population. Additional advantages of CRAT-V include its self-report structure, which makes this tool more accessible and minimizes the amount of training required for practitioners.
Some risk assessment tools, such as the Intimate Partner Violence Assessment Icon Form (IPVAIF), require further evaluation to ensure that they are effective and useful in the assessment of risk with vulnerable populations (e.g., women with varying levels of literacy) (Short & Rodriguez, 2002). Other existing tools, such as the Bridge to Safety (B2S) (Wachter & Donahue 2015), the Danger Assessment for Immigrant Women (DA-I) (Messing, Amanor-Boadu, Cavanaugh, Glass, & Campbell, n.d.; Messing, Glass, & Campbell, 2013), the Multicultural Partner Abuse Short Term Program (MPAST) (Singh, 2005), the Muslim Power and Control Wheel (for example, see Cross 2013), and the Severe Intimate Partner Violence Risk Prediction Scale (SIPVRPS) (Echeburua, Fernandez-Montalvo, de Corral, & Lopez-Goni, 2009), have been developed using a cultural lens and/or adapted for specific cultural groups to capture cultural nuances associated with risk (for example, see Cross, 2013).
Key Findings in Risk Management with Immigrant and Refugee Populations
Risk management involves strategies designed to reduce the risk presented by a perpetrator of domestic violence. These strategies may include such interventions as supervision, counselling to address violent behaviour and/or the attitudes and beliefs underlying violent behaviour, or treatment to address other related concerns such as substance use. Risk management strategies may also include prevention programs that address gender equality to reduce the risk of future violence or escalation in violence.
Research supports the importance of culturally-informed treatment programs for abusive immigrant and refugee men (Echauri, Femántiez-Montalvo, Martínez, & Azkarate, 2013; see also Rana, 2012) and the need for additional dedicated resources for interventions that target men (Ben-Porat, 2010). Additional recommendations for culturally-sensitive interventions include (a) strengthening of informal supports (i.e., family or community), (b) education regarding gender equality, (c) linguistically and culturally-competent outreach services, (d) programming targeting behaviour change (e.g., gender roles), and (e) supports to increase English language proficiency (Taft et al., 2008, p. 179). Community-based prevention and intervention programs, and those that promote critical examination of traditional gender roles, are a “promising approach to preventing [intimate partner violence (IPV)] and altering IPV-supportive attitudes” (Yoshihama et al., 2014, p. 258; see also Brandon & Hafez, 2008; Choi, 2015). Further, recognizing that domestic violence intersects with oppression based on social structural forces is necessary to guide these interventions (Hancock & Ames, 2008).
Zannattino (2012) suggests that conflict resulting from the “disruption of traditional gender roles” post-migration is a key factor in both predicting and preventing domestic violence in immigrant and refugee populations (p. 824). As such, domestic violence prevention and intervention programs that address post-migration stressors and vulnerabilities include resettlement programs as well as social services that address patriarchal beliefs and gender equality and that improve employment opportunities for men (Bui & Morash, 2008). Effective interventions in violent relationships post-migration demonstrate an understanding that “economic stressors and gender ideology are intertwined dynamics of exerting and resisting control” (Morash, Bui, & Santiago, 2000, p. 87). Supports aimed at status anxiety and role reversal would be beneficial when working with perpetrators who hold traditional patriarchal values and beliefs (Min, 2001). Additional risk management strategies within these communities may involve interventions such as mental health services and programs for men to enhance acculturation (e.g., language or employment) and programs to assist couples in achieving similar levels of acculturation (Edelstein, 2013).
Counselling for immigrant and refugee perpetrators should address difficulties in coping with discrimination post-migration, counter-socialization (e.g., gender roles, violence supportive beliefs, or sexual coercion), human rights, conflict resolution, respectful communication, or parenting skills (e.g., what makes a “good” father/man), and substance use (Celaya-Alston, 2010; Liao, 2006; Parra-Cardona et al., 2013; Welland & Ribner, 2010; Yoshihama, Blazevski, & Bybee, 2014). Kim and Sung (2016) argue that “strong extra-legal interventions, such as mandatory education or counseling, should accompany the treatment of IPV offenders” (p. 66). When working with immigrant and refugee groups, Welland and Ribner (2010) also emphasize the significance of addressing unresolved trauma, including Post-Traumatic Stress Disorder (PTSD). Ultimately, prevention and intervention programs should involve “interrupting threatened violence” and changing the meaning of such practices and social dynamics (Korteweg, 2012, p. 148), as well as increased counselling options for men who use violence (Thandi, 2013).
Education is an important risk management strategy within immigrant and refugee populations to address the roots of men’s jealousy, loss of status, and the meanings perpetrators attach to their actions (for example, see Rothman et al., 2007). When working with male perpetrators, being educated about domestic violence generally (e.g., prevalence, forms, severity, and alternatives to violence), as well as the Canadian laws related to domestic and sexual violence, can contribute to efforts to reduce violence (for example, see Helms, 2015; Shalabi et al., 2015; Thandi, 2013). Education can best be accomplished through integrating anti-violence awareness into immigrant settlement and/or employment programs or through partnerships with religious and/or immigrant and refugee specific community supports (Liao, 2002; Shiu-Thornton et al., 2005; Pinzon, 2006; Sullivan, Senturia, Negash, Shiu-Thornton, & Giday, 2005).
Key Findings in Safety Planning with Immigrant and Refugee Populations
Safety planning involves strategies to protect survivors from ongoing or escalating violence. Safety for abused immigrant and refugee women is linked to factors that impact their risk of violence. These factors include migration stress, immigration status, settlement location (e.g., rural versus urban), length of stay in the host country, and levels of acculturation (Hancock & Sui, 2009). These factors should be taken into consideration when developing safety plans for immigrant and refugee survivors from different cultural backgrounds (Hancock & Sui, 2009). Furthermore, immigrant and refugee women’s social location and immigration status are important elements of safety planning because they have implications for their rights and access to services (Ending Violence Association of BC et al., 2011).
Safety planning with immigrant and refugee survivors of domestic violence requires not only that their cultural needs be taken into consideration but also that safety plans identify important items such as legal documentation for survivors and their children. It is also critical that safety planning with immigrant and refugee populations consider safety for women who do not leave their abusers, given the significant barriers to leaving (Midlarsky et al., 2006). Messing et al. (2013) recommend using the Danger Assessment for Immigrant Women (DA-I) to assist immigrant survivors of domestic violence with safety planning, as it considers risk factors for, and experiences of, violence for immigrant and refugee women.
Immigrant and refugee women survivors are likely to require more specific programs, a wider range of supports (e.g., language acquisition, employment skills, education, or housing), and longer shelter stays than non-immigrant women survivors (Bø Vatnar & Bjørkly, 2010). They may benefit from domestic violence support groups and counselling, legal and financial assistance, qualified interpretation and translation services, education, and information and services in their own language. These supports are most accessible and effective when delivered by bicultural/bilingual women service providers (Belknap & Vandevusse, 2010; Dutton et al., 2000; Hass, Dutton, & Orloff, 2000; Rana, 2012; Orloff, 2014; Shiu-Thornton et al., 2005).
In situations where survivors are separating from their abusive partners, immigrant and refugee women often become more vulnerable and isolated, and this reality needs to be addressed in programming (Bui, 2003; Vives-Cases et al., 2014). Some of this can be accomplished through increased support for and/or development of social services that include, but are not limited to, affordable market and social housing, shelters and transitional housing, education for abused women, and employment opportunities (Sokoloff, 2005; West Coast LEAF, 2012), as well as the overall facilitation of social services for these groups (Clifford, Porteous, & Varcoe, 2007).
The literature also emphasizes harm reduction models, culturally-competent services, “macro and micro level structural and economic changes” (Sokoloff, 2008, p. 243), “community-based models of social justice” with a basis in “community engagement and accountability” (Sokoloff, 2008, p. 243), prioritizing social change in addition to social services, and empowerment-based programs and services (see also Ontario Council of Agencies Serving Immigrants, 2006). Access to safe housing and legal services can improve the safety and well-being of women survivors and their children, regardless of immigration status (Cesario, Nava, Bianchi, McFarlane, & Maddoux, 2014).
While mainstream anti-violence services provide specialized support to domestic violence survivors, increasing access to culturally-specific community-based services is key when working with immigrant and refugee groups (for example, see Adam, 2000; Latta & Goodman, 2005). Anti-violence services must collaborate and coordinate with settlement services to enhance the safety of domestic violence survivors. Regardless of whether they work in mainstream or multicultural agencies, service providers need to recognize the culturally- specific barriers that impede help-seeking for survivors (Sokoloff, 2005). Service providers must also consider cultural factors (e.g., norms or values), take language barriers into account when supporting immigrant and refugee survivors, and work to raise awareness about women’s rights and available resources (Midlarsky et al., 2006).
Support services must be expanded and improved to include survivors as active program participants while also considering survivors’ cultural and situational contexts (Zarza & Adler, 2008). Recommendations for expanding services for survivors include promoting culturally- informed coping strategies, developing comprehensive outreach programs, and creating support groups for women from similar cultural backgrounds. Additionally, it is important to recognize that some immigrant and refugee women may not feel safe seeking help and/or protection from formal supports (e.g., police) due to factors such as distrust of law enforcement and/or fear of deportation (Bauer et al., 2000; Rizo & Macy, 2011; Yoshihama, 2002).
The literature emphasizes community-based health promotion to break the silence around domestic violence disclosure as well as culturally and linguistically appropriate services that are interconnected and coordinated (Kim & Sung, 2016; Guruge & Humphreys, 2009; Nilsson et al., 2008). Service providers are also encouraged to advocate for immigrants and refugees experiencing violence and to create culturally-informed and appropriate domestic violence services that draw upon available formal and informal resources and supports (Donnelly, 2015; Hancock, 2006). The development of culturally-informed violence prevention and response initiatives that are aimed at addressing the experiences of abuse in a specific cultural community are also important (Mason, Hyman, Berman, Guruge, Kanagaratnam, & Manuel, 2008).
When working with the diverse and complex cultural contexts of immigrant and refugee populations, it is important to consider the unique lived experiences and needs of each abused immigrant or refugee woman within a holistic framework as well as the cultural and multidimensional dynamics underlying the abuse and creating barriers to safety (Lee, 2000; Sharma, 2007). Support services need to recognize that immigrant and refugee women are often stigmatized in intersecting and complex ways due to race, ethnicity, gender, and immigration status and that providing support requires an understanding of the community and cultural contexts in which they live (Mason et al., 2008). Service providers should recognize and acknowledge the strongly entrenched cultural norms that perpetuate gender inequality and that stigmatize women who leave abusive partners (Mason et al., 2008).
A significant barrier to help-seeking for immigrant and refugee survivors is a lack of awareness about available services, resources, and supports. Education about domestic violence, safety, women’s rights, legislative protections, and available resources and services needs to be made available within immigrant and refugee communities (Ahmadzai, 2014; Battered Women’s Support Services, 2010; Brabeck & Guzmán, 2009; Crandall, Senturia, Sullivan, & Shiu-Thornton, 2005; Guruge & Humphreys, 2009; Fernbrant, Östergren, & Cantor-Graae, 2011; Kulwicki et al., 2010; Lee, 2000; Mason et al., 2008; Moynihan, et al., 2008; Pendleton, 2003; Reina, Lohman, & Maldonado, 2014; Sharma, 2001; Sokoloff, 2005; Sullivan et al., 2005; Taft et al., 2008; Thurston et al., 2013; Trijbetz, 2011; Washington State Coalition Against Domestic Violence, 2011; Yick & Ooman, 2009). Domestic violence education and awareness-raising initiatives must be culturally-sensitive and accessible (e.g., broadcasting on ethnic TV/radio, community outreach in schools and churches, information on public transit and in health centres, or multilingual printed resources; Acevedo, 2000)
Awareness-raising initiatives should be empowerment-focused and address the interconnectedness between domestic violence and hierarchal systems of oppression (e.g., race, class, or gender; Yick & Ooman, 2009). The safety of abused immigrant and refugee women is linked to efforts to mitigate traditional patriarchal power structures and gender roles as well as efforts to build immigrant and refugee women’s sense of agency and autonomy (Battered Women’s Support Services, 2010; Edelstein, 2013; Hyman et al., 2011; Kim & Sung, 2000; Liao, 2006; Marrs Fuchsel, 2014; Taft et al., 2008). Therefore, empowerment-based frameworks must focus on explanations of domestic violence and legal rights, address safety for survivors through referrals and identifying culturally-appropriate services, foster self-esteem, reduce isolation, provide peer support, emphasize healthy and respectful relationships, and provide culturally-relevant and effective interventions (Belknap & Vandevusse, 2010; Fuchsel et al., 2012; Marrs Fuchsel & Hysjulien, 2013; Helms, 2015; Saez-Betacourt, Lam, & Nguyen, 2008; Sheikh, 2008; Shirwadkar, 2004; Trijbetz, 2011). Programs and supports based in empowerment and women’s rights should also be used to address trauma related to domestic and sexual violence in the contexts of war and/or conflict (Zannettino, 2012). Empowerment-based strategies to increase women’s independence and “economic power,” however, need to be coupled with interventions that support men in “abandon[ing] their control efforts” and culturally-defined notions of masculinity (Morash et al., 2000, p. 87).
Culturally-informed domestic violence awareness campaigns should also aim to inform community members and leaders about the risk of domestic violence and homicide at various stages of settlement (Du Mont et al., 2012), and this information should be conveyed in such a way that immigrant and refugee communities can take ownership and action to increase the safety of women and children. Increased community awareness and the capacity to provide practical and emotional support are needed, since immigrant and refugee women experiencing domestic violence are more likely to disclose to informal supports (Donnelly, 2015; Hyman et al., 2006; Kyriakakis, 2014). Furthermore, immigrant and refugee women experiencing violence often access services and supports (e.g., immigration/settlement, medical/health, religious institutions, or cultural and community-based organizations) other than anti-violence services, at least initially (Abu-Ras, 2007; Dutton et al., 2000). This reality calls for an integrated (Natarajan, 2002) and “intersectionally-informed” (Adams & Campbell, 2012, p. 28) service model such that assistance and support broadly, and safety planning specifically, are collaborative and cross-sectoral (Moynihan, et al., 2008). Integrated and collaborative service models require emphasis on informal and community-based supports as well as integrating safety planning and responses to domestic violence into other sectors (e.g., family counselling or nursing programs) in culturally-informed and collaborative ways (Kelly, 2006; Ogunsiji, Wilkes, Jackson, & Peters, 2012; Sokoloff & Pearce, 2011).
Grassroots agencies also need to be involved in increasing domestic violence awareness and acknowledging culture as a source of strength and support for intervention (Ely, 2004; see also Cross, 2013). Interventions must recognize the diverse and intersectional experiences of immigrant and refugee women and must be delivered by culturally-competent service providers who advocate to overcome cultural barriers across multiple systems (e.g., justice, immigration, or child protection; Ely, 2004). Further, cross-sector and multi-agency coordination and collaboration are paramount when working with abused immigrant and refugee women to reduce fear and foster help-seeking (Ben-Porat, 2010; Community Coordination for Women’s Safety, Ending Violence Association of BC, 2007; Ending Violence Association of BC, 2013; Kim & Sung, 2000; Light et al., 2008; Menjivar & Salicido, 2002; Molina, Lawrence, Azhar-Miller, & Rivera, 2009; Rana, 2012; Thurston et al., 2013; Vishnuvajjala, 2012) as well as to enhance holistic, wrap-around services (Light, 2007; Sharma, 2007), with an increased emphasis on culturally-informed safety planning (Gill, 2008).
Service providers who support immigrant and refugee women experiencing domestic violence need to be culturally-competent and culturally and linguistically diverse (Abu-Ras, 2007; Acevedo, 2000; Crandall et al., 2005; Salcido & Adelman, 2004). They must advocate for institutional reforms based on the needs of marginalized survivors including immigrant and refugee women (Sokoloff, 2005) as well as reforms that reflect different communities’ level of awareness of, and sensitivity to, domestic violence (Reina et al., 2014). Practitioners and service providers also need to be educated on specific risk factors and forms of violence (e.g., so-called honour-based violence), so that they are attentive to risks that may inform effective safety planning—without mistakenly seeing these forms of violence as cultural or religious problems (Aujla & Gill, 2014).
Domestic violence risk and safety considerations in immigrant and refugee populations are closely linked to migration, settlement, and acculturation (Berry, 1997, 2005; Hyman & Forte, 2006; Pan, Daley, Rivera, Williams, Lingle, & Reznick, 2006; Sam, 2006). Research on domestic violence and homicide in immigrant and refugee communities addresses the general risk factors, vulnerabilities, and barriers to help-seeking that are relevant to this population (for example, see Baur et al., 2000; Burnman et al., 2004; Guruge & Humphreys, 2009). There is, however, little research focused on risk assessment, risk management, and safety planning strategies that are culturally-informed and tailored to the cultural contexts and needs of immigrant and refugee populations.
While the existing literature provides a general understanding of the vulnerabilities to, and experiences of, domestic violence faced by immigrant and refugee women, more specific research is needed to address the intersecting and multifaceted variances in vulnerability and risk within specific immigrant and refugee groups and cultures, given that immigrant and refugee communities are heterogeneous. More research is also needed to develop and test culturally- informed and specific risk assessment tools to predict severe and escalating domestic violence, as well as the risk of homicide, within immigrant and refugee populations.
Much of the research in this area offers in-depth analyses of the experiences and needs of immigrant and refugee women survivors. More research is needed, however, to understand the depths and complexities of working with male immigrant perpetrators of domestic violence including what works in terms of culturally-informed domestic violence prevention and intervention programs for immigrant men. Furthermore, the literature emphasizes the need for collaborative, cross-sectoral responses (e.g., anti-violence, settlement, child protection, justice, or health) and initiatives to address risk and safety within immigrant and refugee populations generally—including risk management and safety planning strategies. Research addressing the value of collaborative and cross-sectoral responses to domestic violence within immigrant and refugee communities should also be attuned to and specifically explore the role of community and religious leaders, as well as religious institutions, in domestic violence prevention and intervention with immigrant and refugee populations.
Implications for Practice and Policy
Risk assessment, risk management, and safety planning strategies within immigrant and refugee populations need to consider complex and intersecting risk factors both pre-migration (e.g., trauma) and post-migration (e.g., stressors related to settlement and acculturation; Hassan et al., 2011; Shalabi et al., 2015; Taft et al., 2008; West, 2015). Dynamic risk[10] factors are critical to risk assessment, risk management, and safety planning (Brownridge & Halli, 2002). Among immigrant and refugee populations, these factors may include: (a) the impacts of acculturation on experiences of, and increased risk for, violence; (b) the effects of geographic and social isolation on risk of violence; (c) higher levels of independence among immigrant women and/or lower levels of employment among immigrant men, which can create a power imbalance and increased risk of violence; and (d) the relationship between patriarchal ideologies and domestic violence (Brownridge & Halli, 2002).
Practitioners who are assessing and managing risk and developing safety plans with immigrant and refugee populations should be aware that factors such as isolation and marginalization may further inhibit women’s ability to seek protection from police and access support services and health care. Thus, service providers working with immigrant and refugee populations must be able to recognize risk factors within these populations (Messing et al., 2013).
Strategies to address risk and safety must focus not only on individual and relationship levels, but also on community and structural levels (Hyman et al., 2011). Effective strategies to address the intersecting issues linked to risk and safety within these populations must include interventions at all levels. For example: (a) offering culturally-appropriate education and counselling and strengthening of connections to reduce social isolation (i.e., individual, relationship, community levels), (b) addressing victim-blaming and racist attitudes and challenging gender inequality (i.e., community, social levels),and (c) increasing access to child care, recognizing foreign credentials, improving training and employment opportunities, and offering English language classes (i.e., structural level) (Hyman et al., 2011).
Intersections of gender, migration, culture, and religion add layers of complexity that impact how domestic violence is understood, experienced, reported, and responded to within immigrant and refugee populations (Hancock & Sui, 2009). Many cultures place value in family unity and cohesion, and some researchers suggest that prevention and intervention strategies may be more effective if they reflect core cultural values (Baobaid, n.d.; Chokshi, 2007; Sabri et al., 2015). Research suggests that the efficacy of interventions among this population can be enhanced by involving family and community members, religious leaders, and friends (to provide informal support and resources) and reinforcement of family norms and cohesion (Brabeck & Guzmán, 2009; Shalabi et al., 2015). Conversely, Natarajan (2002) found that involving extended family members increased the risk of domestic violence for immigrant women from India. As such, in working with domestic violence victims/survivors from diverse cultural groups, it is important to consider how family unity and cohesion, as well as involving extended family members, may serve as risk and/or protective factors.
A consistent theme throughout the literature on prevention and intervention with respect to domestic violence in immigrant and refugee populations is the need for culturally-informed and appropriate interventions and supports aimed at specific groups or cultures. To access these populations and effectively prevent and/or intervene in cases of domestic violence, there is a need to provide specific supports and services (e.g., bilingual and multicultural) to groups from different ethnic and religious backgrounds (Klevens, 2007; Sokoloff, 2005). For example, Klevens (2007) advocates for cross-sector collaboration to develop culturally-appropriate interventions through knowledge sharing, cultural competency, and increased language capacity of services for non-English speaking clients (see also Ahmadzai, 2014). Culturally-informed approaches can be used to enhance the effectiveness of interventions (e.g., respectful relationships, healthy communication, family systems therapy, or couples counselling), raise awareness about domestic violence, and enhance problem-solving skills (Lee, 2000; Klevens, 2007). Within the diverse cultural contexts of immigrant and refugee groups, multi-organizational interventions are also essential to developing and delivering culturally-appropriate interventions (Lee, 2000).
Culturally-informed prevention and intervention programs should address gender-based violence by fostering cultural resiliency (Shalabi et al., 2015). Effective interventions based in cultural resiliency are recommended and build on cultural strengths and norms by using religiosity, family beliefs, autonomy, and recognition of gender roles. Similar approaches are seen in research emphasizing culturally-informed interventions, counselling, and services for immigrant male perpetrators (Abu-Ras, 2007) and immigrant and refugee communities in general (Pan et al., 2006; Yick & Oomen, 2009). For example, Sigal (n.d.) recommends developing culturally-informed and multi-factor interventions to address the complexity of violence in immigrant and refugee communities and its interconnectedness with various components of different cultures.
The common vulnerabilities that compromise the safety of immigrant and refugee women in general, as well as the cultural variables that distinguish their experiences from one another, emphasize the importance of understanding and contextualizing risk, safety, prevention, and intervention within individual and cultural contexts. Furthermore, these vulnerabilities also support the need for culturally-appropriate and informed services and system responses. Failure to adequately examine and address the needs, risks, and vulnerabilities of immigrant and refugee survivors broadly, as well as distinct cultural groups, further compromises the safety of this population and increases their risk of experiencing severe, escalating, and potentially lethal forms of violence.
Children Exposed to Domestic Violence
Authors: Laura Olszowy, Mike Saxton, Katherine Reif, Marcie Campbell, Peter Jaffe
Contributors: Myriam Dube, Katreena Scott, Wendy Verhoek-Oftedahl, Jordan Fairbairn
The adverse impact of the exposure to domestic violence on children’s development is well-documented in the literature (Jaffe, Wolfe & Campbell, 2011; Holt, Buckley, & Whelan, 2008; Wolfe, Crooks, Lee, Macintyre-Smith & Jaffe, 2003). However, what is less understood is the risk for lethality faced by children living with domestic violence. While there are tools for assessing lethality risk of adults in situations of intimate partner violence, these tools do not specifically address the risk to children living within these circumstances. Knowledge about lethality risk factors for both adult and child victims can provide professionals with the necessary information to develop safety plans with adult victims as well as guide risk management interventions with those individuals perpetrating the violence; this then helps to keep both adult and child victims safe.
According to the 2008 Canadian Incidence Study of Child Abuse and Neglect, child exposure to domestic violence includes direct or indirect exposure to both physical and emotional violence. Direct exposure is where the child is physically present and witnesses the physical and/or emotional violence between intimate partners; indirect exposure includes situations where the child overhears or sees some of the immediate consequences of the abuse (e.g., injuries to the mother; Trocmé et al., 2010). In Canada, child exposure to domestic violence is one of the most frequent forms of maltreatment, accounting for 34% of substantiated cases annually (Trocmé et al., 2010). Similar to other forms of maltreatment, infants and toddlers are disproportionately at-risk for exposure to domestic violence. Approximately 25% of children investigated for direct exposure to domestic violence are between one and three years of age, and a further 10% of exposed children are under the age of one year (Trocmé et al., 2010).
Children living in homes where domestic violence is present are considered vulnerable for many reasons. Over half of maltreatment cases based on evidence of exposure to intimate partner violence involved multiple incidents of contact with child protection services (Trocmé et al., 2010). Children exposed to domestic violence are also at-risk for physical harm. In Canada, children comprise 39% of those physically injured by the perpetrator in domestic violence cases before the court (Beaupré, 2015). Children may also attempt to protect their mother from the perpetrator during an abusive incident. In a study of 110 domestic violence victims across four U.S. cities, approximately 1 in 4 children became physically involved as the abusive incident was occurring (Edleson, Mbilinyi, Beeman & Hagemeister, 2003).
Child victims of domestic violence may not always be reported to the authorities. Infants and young children, for example, are not capable of reporting victimization themselves. Furthermore, older children and youth may be reluctant to contact the police due to fear of reprisal and/or dependency on the perpetrator (AuCoin, 2005; UNICEF, 2011). Research has also shown that children living in unstable financial and social environments are more likely to intervene and call for help, underscoring the relationship between family stability as a risk factor and children’s willingness to seek help (Edleson et al., 2003). In other words, children exposed to domestic violence who live in otherwise more stable financial and social environments may be more reluctant to seek help, thereby placing them at-risk for harm. As well, research suggests that police officers responding to domestic violence are often reluctant and/or have a lack of confidence speaking to children, and they do not always view children as central victims in domestic violence incidents (Richardson-Foster, Stanley, Miller, & Thomson, 2012). This dynamic may ultimately compromise children’s safety in the context of domestic violence, as children are reluctant to report to the police and officers may have difficulty interacting with children.
In extreme cases, children are killed in the context of domestic violence. These cases differ from child maltreatment-related homicides, as they are more likely to occur in the context of separation and as an act of revenge (Jaffe & Juodis, 2006; Dawson, 2015). Child homicides in the context of domestic violence may not be readily identified or subject to consistent definitions in research (Fairbairn et al., 2017).
For the purpose of our literature review, child domestic homicide is defined as follows:
- child(ren) killed as a result of intervening during a violent episode between parents;
- child(ren) killed by a parent as revenge against the partner (e.g. partner ended relationship or other perceived betrayal);
- child(ren) killed by a parent as part of a murder-suicide;
- child(ren) killed by parent with a history of domestic violence (e.g. perpetrator of child homicide was a victim and/or perpetrator of domestic violence; or
- child(ren) killed by a third party (e.g., older sibling) at the direction of a parent.
For this definition, “parent” includes biological parent, step-parent, foster parent, and/or other caregivers (e.g. mother/father's new intimate partner or other family member acting in a caregiving role). A history of domestic violence refers to an official (e.g., police reports) or unofficial (reported by friends, family members) history of domestic violence in the current relationship. Child is defined as a person who is under the age of 18. Cases wherein an individual under the age of 18 is killed by an intimate partner (e.g., dating relationship) are not part of the definition of child domestic homicides.
Domestic Violence Death Review Committees (DVDRCs) or related government inquiries have reported on trends and risk factors associated with child deaths across Canada, the U.S., Australia, New Zealand, and the U.K. In Canada, several committees have examined cases of children killed where a history of domestic violence was present. Specifically, Ontario identified 36 children who were killed between 2002 and 2014, and Alberta identified 11 children who were killed between 2008 and 2014 (Ontario DVDRC, 2015; Alberta Family Violence Death Review Committee, 2015). These findings stress the importance of recognizing the vulnerability of children when developing risk assessment, safety planning, and risk management strategies in cases of domestic violence. Findings and their implications for research and practice in this area are discussed below.
Key Findings in Risk Assessment with Children Exposed to Domestic Violence
Risk Factors. The assessment of lethal risk posed to children living in homes with domestic violence is a challenging undertaking. It is difficult to identify risk factors specific to the risk of child homicide. Research has identified several common interrelated risk factors that increase the likelihood of an intimate partner relationship becoming lethal, most significantly a history of domestic violence and actual or pending separation (Kropp, 2008; Ontario DVDRC, 2015). However, what remains unclear is the risk factors that specifically place a child at-risk for lethality (Jaffe, et al., 2012; Humphreys & Bradbury Jones, 2015). The literature acknowledges the complex nature of assessing risk with families experiencing domestic violence (Fleck-Henderson, 2000; Hughes & Chau, 2013; Radford et al., 2006; Shlonsky & Friend, 2007). One study that examined data collected from domestic homicide case reviews in Ontario found no factors that differentiated cases where children were killed from cases where children were not killed, aside from the fact that there were significantly more community service agencies involved with the family prior to the homicide (e.g., schools, family court, or child protection) in cases where children were killed (Hamilton, Jaffe & Campbell, 2013).
In the literature on safeguarding children living with domestic violence, parental separation is well-documented to be a time of increased risk for lethality and severe violence (Bragg, 2003; Humphreys & Bradbury Jones, 2015; Kirkwood, 2013; Lessard et al., 2010; Wendt, Buchanan & Moulding, 2015). A few similar studies have identified in perpetrators the presence of mental health issues (e.g., depression or psychosis) often prior to the homicide (Jackson, 2012; Sillito & Salari, 2011; West, 2009). An examination of predictors of child outcomes in 325 intimate-partner homicide-suicide cases in the U.S. from 1999-2004 found that in cases where children were killed (a) a slightly higher percentage had parents in an intact relationship; (b) children were more likely to be killed by perpetrators with primarily suicidal intent; and (c) they were more likely to be the biological child of the perpetrator (Sillito & Salari, 2011). Outside of these studies, there remains a relative dearth of research examining the risks of children being killed in the context of domestic violence (Hamilton et al., 2013; Olszowy, Jaffe, Campbell, & Hamilton, 2013).
Risk Assessment Tools. There is a lack of standardized risk assessment tools that assess for the risk of child lethality in the context of domestic violence. While there are many tools that assess risk for lethality of the adult victim, tools that specifically assess for risk of child lethality are not available (Olszowy et al., 2013). A study that examined the utility of commonly-used tools (Danger Assessment (DA), ODARA, and B-SAFER) for assessing risk of lethality and severe domestic violence did not differentiate overall risk for cases where children were killed compared to cases where children were present but not killed (Olszowy et al., 2013). Individual items on the DA (prior threats to harm children) and the B-Safer (relationship problems) were associated with child domestic homicides. Another tool, Barnardo’s Domestic Violence Risk Identification Matrix, has been named as a promising tool for identifying risk to children living with domestic violence (Healey & Bell, 2005; Stanley & Humphreys, 2014). However, it is not specific to risk for lethality and lacks research on the tool’s reliability and validity.
The most consistent finding acknowledged in the literature with respect to child risk for lethality in domestic violence cases is that an intimate partner’s risk for lethality is parallel to their child’s risk (Black, Dempsey & Davis, 2010; Bourassa, Lavergne, Damant, Lessard, & Turcotte, 2006; Cooley & Frazer, 2006; Hamilton et al., 2013; Lake, Odom, & Starsoneck, 2003). This finding, coupled with the finding that there were significantly more community service agencies involved with the family in cases where children were killed, suggests implications for community service providers who are aware of children living with a parent also at high risk for lethality (Hamilton et al., 2013).
The Role of Community Professionals in Identifying the Risk for Lethality. Domestic violence reports involving children often trigger system responses from child protection, law enforcement, the courts, and violence against women sectors. Increasingly, professionals working in these separate sectors understand the importance of communication and collaboration when it comes to identifying risk (Cooley & Frazer, 2006; Coulter & Mercado-Crespo, 2015; Cross, Matthews, Tonmyr, Scott & Ouimet, 2012; Shlonsky & Friend, 2007). The driving force towards communities developing coordinated service approaches has come from the domestic violence death review findings that highlight the shortcomings of services operating in siloes (Hamilton et al., 2013; Jaffe & Juodis, 2006)
Research has emphasized that a mother’s risk for lethality is inextricably tied to her child’s risk (Humphreys et al., 2001). Previous research with mothers has identified that professionals, in order to be able to gather information to assess risk, must build trust with the mother and her children (Lapierre & Côté, 2011; Lavergne et al., 2011; Varcoe & Irwin, 2004). Research examining children’s and parents’ perspectives when engaging with service providers regarding DV revealed that children, victims, and perpetrators highlighted the importance of agencies and police officers taking them seriously, validating their perspectives, remaining non-judgmental, and being able to intervene effectively (Stanley, Miller, & Richardson-Foster, 2012). Additionally, an understanding of the dynamic risk factors in DV cases is crucial for developing and adjusting safety plans. For example, separation heightens the risk for lethality for adult victims significantly (Brown & Tyson, 2012). Existing research highlights the importance of understanding dynamic risk factors when considering the impact of safety of all family members (Cooley & Frazer, 2006; Hardesty & Chung, 2006).
Child Protection Services. Living with domestic violence may be considered a form of psychological maltreatment and trigger a mandatory report to child protection. Therefore, child protection services are central to assessing risk for these children. Exposure to domestic violence is one of the leading kinds of reports to child protection services across Canada (Public Health Agency of Canada, 2010). These services determine if children are at-risk and in need of protection. The execution of this role may vary widely across jurisdictions.
Extensive research has been conducted on child protection practice and interventions with families experiencing domestic violence in North America (Button & Payne, 2009; Hughes & Chau, 2013; Hulbert, 2008; Lapierre & Côté, 2011; Lavergne et al., 2011; Jenney, 2011; Mills et al., 2000; Pennell, Rikard & Sanders-Rice, 2014; Postmus & Merritt, 2010; Radford, Blacklock & Iwi, 2006; Shlonsky & Friend, 2007). Child protection services have focused their interventions on reported concerns directly related to children being harmed (e.g., physical or sexual abuse allegations). In recent years, there is recognition that living in a home where intimate partner violence is occurring can place children at-risk of harm. In fact, rates of co-occurrence of intimate partner violence exposure and other forms of child maltreatment range, with rates of 60-75% commonly cited (Wathen & MacMillan, 2013). Professionals in child protection may not always accurately identify the presence of DV (Bourassa et al., 2006; Kohl, Barth, Hazen, & Landsverk, 2005; Rivers, Maze, Hannah, & Lederman, 2007). Obstacles to child protection workers effectively detecting DV in families may include parents’ denial, lack of evidence, heavy workloads of workers, lack of cooperation by parents, short duration of interventions, and parental substance abuse (Bourassa et al., 2006; Kohl et al., 2005). The barriers to accurately identifying DV has implications for assessing the risk for lethality that children may face.
Risk assessment tools utilized in child protection are not specific to risks posed by domestic violence (Jenney, 2011; Shlonsky & Friend, 2007). Domestic violence may be one factor that child protection workers consider as part of their standards of practice for assessment, but DV as a single risk factor may not influence their decision making (Hughes & Chau, 2013). While child protection workers may base their assessments and interventions on factors typically included in risk assessment tools, they engage in a complex decision-making process regarding risk to children, how violence impacted them, and the caregivers’ willingness to accept responsibility and make changes (Hughes & Chau, 2013). In their review of the literature on the utility of risk assessment tools in the context of child maltreatment and DV, Shlonsky and Friend (2007) articulate that good risk assessment instruments are better with prediction than clinical judgment, though the worker plays a crucial role in assessing the dynamic context of child maltreatment and DV. Standardized risk assessment tools for DV not having been tested with child protection clients limits their potential validity within this sector.
The child protection role in assessing risk in families where there is domestic violence has not been clear (Jenney, 2011; Kohl et al., 2005; Postmus & Merritt, 2011; Radford et al., 2006; Shlonsky & Friend, 2007). Personal (e.g., demographic characteristics) and professional factors (e.g., prior case experience; or agency policies and protocols) can influence child protection worker’s beliefs about domestic violence and subsequently their response (Postmus & Merritt, 2010). Child protection workers may have more knowledge of domestic violence than other social service workers, but they may have insufficient knowledge about communicating the risks for lethality and interventions with perpetrators (Button & Payne, 2009). Concerns have been expressed that child protection interventions may expose victims to further risk (Button & Payne, 2009).
Depending on how the level of risk to the child is conceptualized (e.g., directly or indirectly harmed, physically or emotionally), child protection workers may not remain involved with the family and thus miss the opportunity to address dynamic risk factors (Hughes & Chau, 2013). One study, which looked at the response of child protection workers and the factors involved in deciding to keep a case open for ongoing service or remove a child from the home, found that DV by itself is not a factor that influences the decision to keep a case open or lead to more intensive intervention (Lavergne et al., 2011). Rather, the response by child protection services seemed to be more influenced by the presence of other forms of maltreatment and risk factors including the severity of the maltreatment and parental risk factors (Lavergne et al., 2011).
The child protection sector is uniquely positioned to intervene with fathers. In some cases with no criminal court involvement, they are the only mandated service provider. However, mothers are more often held responsible for the supervision and safety of children than are fathers (Hartley, 2004; Hughes, Chau, & Poff, 2011). Research with mothers who experienced intimate partner violence and who were involved with the child protection system showed that mothers felt that child protection workers put the responsibility for their partners’ violence solely on them (Hughes et al., 2011).
Best practices for assessing risk for lethality within child protection services have not been well-documented in the literature and may in fact not be well-developed and vary amongst communities. Additionally, it has been argued that the field of child protection has been slow to realize that helping establish safety for the mother is synonymous with ensuring safety for the children (Hughes et al., 2011; Shlonsky & Friend, 2007). Some research suggests that the child protection system may even be reluctant to become involved for fear that they are being drawn into a child custody dispute with conflicting allegations (Lessard et al., 2010).
Police Services. Police are often the first responders when there is a domestic dispute and may be the first professional that has contact with the family. Police have a crucial role in initial assessment of risk and intervention for children living with DV (Baker, Jaffe, Berkowitz & Berkman, 2002). However, police may have limited training in dealing with the impact of exposure to DV on children (Richardson-Foster et al., 2012). A qualitative study on police intervention in DV cases in the U.K. found that police officers often lack confidence speaking to children at a DV incident. Police may feel that intervention with children is not part of their job or that they lack the appropriate resources to engage with children (Richardson-Foster et al., 2012).
Another study that examined police notifications of incidents of domestic violence to child protection services and the communication between these two services found that the police conveyed very little information on the children’s experiences of domestic violence, including information on risk (Stanley, Miller, Richardson-Foster, & Thomson, 2010). Clear identification of risks faced by children is critical when reporting to child protection services (Baker et al., 2002). Although police may be aware of the factors that meet the threshold to report to child protection services, research has demonstrated that police officers are least likely, compared to other professionals working with cases of domestic violence and child maltreatment, to identify and report indicators of domestic violence (Spath, 2003).
Violence Against Women Services. The literature on assessing risk for children by professionals in the violence against women (VAW) sector is limited. While VAW workers may include children as part of their risk assessment, the primary focus is on the adult victim. Typically, professionals in the VAW sector play a role in contacting the appropriate services for children and maintaining continued collaboration with professionals involved with children.
Courts. Cases of DV can enter the justice system through one or more doors in Canada: the criminal, family, or child protection court systems. Families involved with the justice system will likely go through DV screening or undergo a more formal risk assessment (Department of Justice, 2013). Given the different objectives and legal standards of these three systems, professionals working in these systems face challenges when assessing risk especially when information is not shared (Johnston, 2006). Failing to properly share information among the family, criminal, or child protection systems hinders the ability to complete a comprehensive risk assessment. Moreover, the use of risk assessment tools is not consistent across Canadian jurisdictions (Department of Justice, 2013). The absence of information sharing among the systems responding to DV cases lessens the likelihood of consistent identification or awareness of the potential risks. Additionally, there is not consistent DV screening in the family law system. U.S. research has found a lack of routine identification of DV victims accessing the family law system during child custody proceedings (Hardesty & Chung, 2013).
Professionals in Healthcare and Education. Professionals in settings such as healthcare and education play a role in the early detection of DV and assessment of risk. Primary prevention programs, such as home visitation and support programs, to families with young children present an opportunity for professionals to detect DV (Kan & Feinberg, 2014). Studies on early childhood home visitation and support programs demonstrate that it may be a strategy for reducing intimate partner violence particularly for families with children at risk of maltreatment (Asawa, 2008; Bair-Merritt et al., 2010; Chamberlain, 2008; Kan & Feinberg, 2014).
School personnel are in an ideal position to recognize the signs and symptoms of DV and tend to understand their mandatory reporting obligations. However, educators may not fully understand their role in helping child victims of DV. A study examining the effectiveness of a DV training program for school settings found more than one-third of respondents were unaware of their school’s policies and procedures related to DV, and half were unsure of the resources available to victims in the community even after the training program (Young, Mancuso, Faherty, Dorman, & Umbrell, 2008).
Screening for DV in healthcare settings is a widely researched and debated issue (Wathen & MacMillan, 2013). A review of the literature found universal screening for DV experienced by women to be ineffective for reducing subsequent violence; however current best practice guidelines in Canada recommend that practitioners be alert to specific indicators of DV and assess for emotional and behavioural problems in children (Wathen & MacMillan, 2013). Professionals in pediatric settings are uniquely situated to identify risks for children and to be aware of the mandatory reporting standards in their jurisdictions when child maltreatment is suspected (Black et al., 2010; Schilling, Snyder & Scribano, 2012; Wathen & MacMillan, 2013).
In many regions, it is not routine to screen for DV in pediatric settings (Schilling et al., 2012). Research demonstrates that family violence assessments allow for more complete health care for children (O’Malley, Kelly & Cheng, 2013). Though mothers may be reluctant to discuss DV with physicians for fear of losing their children, one study revealed that women would like DV screenings to be conducted even if they did not disclose DV (Wathen & MacMillan, 2013; Zink, 2000). However, the approach a health care practitioner takes to discuss DV is critical (Zink, 2000). There are barriers to effectively screening for DV within these settings. Studies conducted with practitioners reveal that many lack knowledge about what to do following a positive screen for family violence (Borowsky & Ireland, 2002; Schilling et al., 2012). Other factors, such as lack of time, privacy, knowledge/training, staff, fear of offending the caregiver or victim, and beliefs that exposure to DV does not impact a child’s well-being, have been cited by healthcare practitioners as barriers to effective DV assessments (O’Malley et al., 2013; Schilling et al., 2012).
Key Findings in Risk Management with Children Exposed to Domestic Violence
Risk management in the context of domestic violence (DV) for children has been the subject of limited research. While it is widely recognized that children can be secondary victims of a domestic homicide, empirical evidence supporting any particular approach to risk management is lacking (Hamilton et al., 2013; Jaffe et al., 2014). Literature suggests risk management strategies are frequently dependent on the nature of the violence, access to appropriate and available resources, as well as the immediate situation and environment (Nixon et al., 2015). Research has focused on examining risk management strategies in the context of preventing reoccurrence of DV victimization rather than lethal violence. As such, this section largely examines key findings that emerged when reviewing the literature on risk management strategies for DV and childhood exposure to DV.
Separation and Risk Management. Actual or pending separation between DV victims and perpetrators increases the likelihood of a domestic homicide to occur (Kropp, 2008; Ontario DVDRC, 2015). Separation as an intervention goal may not always be in the best interest of victims and their families when developing a safety plan (Stanley et al., 2012; Hardesty & Chung, 2006; Humphreys & Bradley-Jones, 2015). Separation becomes increasingly more complex when children are present due to the potential conflicts over custody and access of the children (Lessard, 2010). Ironically, interventions with families experiencing DV are often withdrawn when there is an acknowledgment that the couple has separated with the assumption that the problems have become legal rather than clinical or social service issues (Stanley, 2010).
Custody, Access, and Supervision. Managing risk after separation is confounded by child custody and access disputes. Custody and access conflicts create a problematic source of contact between DV victims and their abusers (Varcoe & Irwin, 2004). While joint custody or shared parenting has been suggested to be the most favoured option for separating parents, this plan may be dangerous in high-risk DV situations (Hardesty & Chung, 2006; Horn, & Groves, 2006; Lessard, 2010; Olszowy et al., 2013; Jaffe et al., 2009). DV perpetrators may be at a higher risk for child maltreatment (Johnston, 2006). However, studies have found that protection of both victims and children can be both ignored and minimized throughout the process of child contact coordination in DV cases (Humphreys & Harrison, 2003); moreover, women can find these to be sites of ongoing DV victimization. Researchers have found a lack of consistent screening for DV, little assessment of risk, a poor understanding of conflicting reports about DV, and limited secure child access centres as particular barriers to effective contact plans for children (Humphreys & Harrison, 2003). Many courts ignore domestic violence as a primary consideration in custody and access decisions (Saunders, 2007). More empirical research is needed to examine the complex intersection between custody, access, domestic violence, and the risk for lethality (Saunders, 2007).
Role of Child Protection Workers. There have been repeated calls for child protection professionals to develop skills in engaging with domestic violence perpetrators to support the safety of victims and children (Jenney, 2011; Stanley et al., 2010). Research on child protection workers’ perspectives on their services has identified a lack of training to specifically examine managing DV perpetrators’ behaviours (Jenny 2011; Stanley et al., 2010). Furthermore, child protection workers have expressed difficulties working with perpetrators of DV and point to the limited resources at their disposal to work with violent men (Lapierre & Côté, 2011). While there have been positive gains by child protection workers working with victims of DV, the literature overall indicates that child protection workers need continued training, supervision, and support aimed at increasing skills and confidence in working with perpetrators of DV (Stanley et al., 2010).
Parenting Programs. Research has highlighted the importance of engaging men as fathers to help overcome past history of DV (Pennell et al., 2014; Stanley et al., 2012; Wendt et al., 2015). Men who persevere in addressing their past behaviours and engage with interventions may do so in part due to their desire to be close to their children (Pennell et al., 2014). Therefore, exploring the extent of children’s exposure to DV may provide a useful starting point for engaging violent fathers (Stanley et al., 2012). This perspective has led to innovative models of treatment that are focused on perpetrators’ role as parents and that have been developed as potential risk management strategies. One such intervention geared toward engaging fathers is the “Strong Fathers” program, a psychoeducational fathering program for men who had committed DV and who were referred by child protection (Pennell et al., 2014). An early analysis of the Strong Fathers program found a decrease in child protection contact and less self-reported violence within the home upon completion of the program (Pennell et al., 2014).
Early Intervention and Co-Parenting. Early intervention is crucial in any risk management strategy. Research identifies that children under the age of five are at an increased risk of being exposed to domestic violence, and findings support early intervention efforts that target families around the birth of a new child (Gustafsson, Cox, & the Family Life Project Key Investigators [FLPKI], 2016; Gustafsson, 2013). One such initiative is the “Family Foundations” program (FF), a psychoeducational program developed to support new parents in caregiving as well as to increase positive communication between partners (Kan & Feinberg, 2014). A longitudinal evaluation examining FF program’s impact on partner aggression found a reduction in risk factors related to family violence as well as in domestic violence and child abuse. These reductions were accompanied by an increase in more positive and mitigating factors to partner violence (i.e., reducing parental stress and depression, enhancing co-parenting, improving children’s social competence, and reducing children’s behaviour problems; Kan, & Feinberg, 2014). These findings have led researchers to point to the vital role that proactive interventions may contribute to reducing DV (Kan, & Feinberg, 2014).
Key Findings in Safety Planning with Children Exposed to Domestic Violence
Safety Planning with Mothers AND Children. Safety planning for mothers and their children is critical to the prevention of domestic homicide. As an illustration of this point, a U.S. study on abuse victims found that one-quarter of the mothers reported their children were physically involved when violence was committed against their mothers (Edleson et al., 2003). Safety planning for children exposed to domestic violence may be conducted by workers in the domestic violence and child protection sectors. In many jurisdictions, safety planning by child protection workers is a structured and mandatory response to a child protection referral (Fleck-Henderson, 2000; Jenney, 2011). Within the VAW sector, safety planning is often undertaken with the adult victim following a disclosure of domestic violence. Victim safety planning may be conducted by victim service providers, shelter workers, police, family services, and family justice officials (Department of Justice Canada, 2013). Much of the literature suggests that effective safety planning should include both the mother and her children along with cross-disciplinary collaboration that is guided by risk assessment (Kohl et al., 2005; Waugh & Bonner, 2002). Several authors have highlighted the need to develop differential plans that respect the adult victim’s autonomy yet place children’s safety at the forefront—depending on the severity of violence and degree of coercive control tactics (DeVoe & Smith, 2003; Jaffe, Crooks, & Bala, 2009).
Within the child protection sector, safety planning for children living with domestic violence depends on information gathered from an overall risk assessment of maltreatment. Jenney (2011) suggests that child protection workers should consider differentiating domestic violence cases from other forms of child maltreatment to expand the narrow view of what constitutes safety (i.e., leaving the abusive relationship) and to incorporate more pragmatic solutions to improving the safety of women and children (i.e., engaging with men to end abusive behaviours). Further, it is suggested that child protection workers need to recognize the complexity of risk assessment and safety planning and then use this knowledge as a means of working domestic violence cases more collaboratively with other service providers (Jenney, 2011).
Safety planning may depend on an analysis of dynamic and static risk factors. Separation is a dynamic factor that may elevate risk and therefore needs to be specifically addressed in a safety plan (Brown & Tyson, 2012; Jaffe et al., 2015). Several authors have pointed to the importance of creating standardized safety plans with some flexibility to recognize risk factors (Horton et al., 2014; Jaffe et al., 2015; Thomas et al., 2015). There is a close relationship between the safety of the mother and the safety of her children (Hughes et al., 2011; Shlonsky & Friend, 2007; Wendt et al., 2015). Keeping children safe in cases where domestic violence is present requires a thorough assessment of the nature of the risk factors they face. A study conducted in the U.K. on police engagement with domestic violence calls found that increased interaction and attention to children and adolescents at the scene can enable reassurance and the provision of appropriate resources to the child (Richardson-Foster et al., 2012). Although much of the literature offers advice and guidelines for professionals in the field, there is little empirical evidence to support one form of safety planning over another.
Safety Plans for Children. While safety planning often focuses on working collaboratively with the mother to keep her and her children safe, several authors have supported the importance of working with children to develop developmentally appropriate safety plans (Chanmugam & Hall, 2012; Kress et al., 2012; MacMillan, Wathen, & Varcoe, 2013). The goals of safety planning with children and youth are primarily centered on addressing physical and emotional safety, with some emphasis on preventing future dating violence for youth (Chanmugam & Hall, 2012). Research conducted with shelter workers in the U.S. found that more than 75% of respondents completed safety planning with children and/or youth individually (Chanmugam & Hall, 2012). The authors highlight the need for ongoing safety planning with children and youth that considers their developmental differences and is guided by the child’s ideas, decisions, and what has worked for them in the past, delivered using multiple methods (Chanmugam & Hall, 2012).
Some of the U.S. research on safety planning has focused on interventions designed to teach preschool aged children exposed to domestic violence about safety plans (Preschooler Kids’ Club). This research found that the majority of children had minimal safety planning strategies at baseline, and many in both the intervention and control group failed to provide safety responses post-intervention (Miller, Howell, Hunter, & Graham-Bermann, 2012). The authors suggest that the results indicate (a) safety plans should be presented using developmentally appropriate strategies that foster a sense of mastery in each child (e.g., role-playing) and (b) safety planning should be explicitly taught to mothers as well to facilitate the child’s learning.
Many researchers highlight that children must clearly receive the message that the prevention of violence is the responsibility of the adult, not the child. Children can be educated on the importance of staying safe and not trying to intervene directly in a manner that puts them at further risk of harm (Baker et al., 2002; Sillito & Salari, 2011). In fact, one study evaluated the outcomes for 58 children and youth involved in an intervention program for witnessing domestic violence (The Child Witness to Violence Program). This program is designed to improve their understanding that the violence was not their fault and to increase their awareness and knowledge of safety planning (Ernst, Weiss, Enright-Smith, & Hansen, 2008). Results indicated significant post-intervention improvement in the number of children who did not take responsibility for the violence and who had increased knowledge in the creation and usage of safety plans (Ernst et al., 2008). From the studies mentioned above, it is clear that developing safety plans with children that are developmentally appropriate and individualized are integral to their safety in the context of domestic violence.
Safety Planning within Context of Child Custody and Access Disputes. Safety planning can be complicated further within the context of child custody and access disputes. In these cases, family law presumptions regarding the need for children to have a relationship with both parents must be balanced with safety planning for women and children (Wendt et al., 2015). A challenging component to safety planning in these cases occurs when the dynamics of domestic violence is playing out in family court. Custody evaluators may not be adequately trained to make recommendations that address the history and impact of domestic violence on the children’s ‘best interests’ (Drozd, Kuehnle & Walker, 2004). A study that evaluated a program designed to enhance safety of children exposed to domestic violence and high conflict custody and access disputes (Speaking for Themselves) found that a model which incorporates therapeutic and legal support to children is beneficial towards improving their safety and sharing their perspectives in these cases (Fotheringham, Dunbar, & Hensley, 2013).
Based on the findings from this literature review, there needs to be a more rigorous focus on risk assessment tools that may be most effective in predicting risk of harm to children. It is too early to decide if separate tools need to be developed or if existing adult tools can be adapted for assessing child risk. As well, there is a need for the evaluation of the effectiveness of safety planning and risk management interventions currently utilized with victims, perpetrators, and their children. While some studies have focused on the effectiveness of intervention programs with children (Ernst et al., 2008; Fotheringham et al., 2013; Miller et al., 2012), there is a clear need for research that evaluates the effectiveness of parenting interventions for victims and perpetrators.
Additionally, there is a need to further examine the system factors associated with child homicide in the context of domestic violence. Different professionals may see children at different points in time related to community and/or court interventions. Some of these interventions may be voluntary and some may be mandatory (e.g., police or child protection services). The identification and disclosure of risk factors may vary by system. Some research conducted on risk factors specific to child lethality has identified separation and divorce (Bragg, 2003; Humphreys & Bradbury Jones, 2015; Kirkwood, 2013; Lessard et al., 2010; Wendt et al., 2015) and issues surrounding perpetrator mental health (Jackson, 2012; Sillito & Salari, 2011; West, 2009) to be particularly important in addressing the prevention and intervention of child homicides. Risk factors and interventions may have to be examined over time from the point of initial disclosure and crisis to many years later in the context of child custody disputes or criminal proceedings. Monitoring risk over time rather than at one point in time would be a challenging enterprise.
Implications for Practice and Policy
Much of the research in this area culminates in recommendations for professionals working with victims, perpetrators, and their children. The most important finding reiterated throughout the literature is that children need to be considered and included in risk assessment, risk management, and safety planning when professionals are working with families experiencing domestic violence (Black et al., 2010; Bourassa et al., 2006; Cooley & Frazer, 2006; Hamilton et al., 2013; Lake et al., 2003).
Training on (a) the dynamics of domestic violence, (b) the co-occurrence of domestic violence and child maltreatment, and (c) barriers to reporting domestic violence is critical to improve the response to children living with domestic violence. One recent study of service providers in Florida found that child protection workers felt less confident about dealing with the dynamics of intimate partner violence (Coulter & Mercado-Crespo, 2015). Moreover, a similar study in Virginia found that while child protection workers had more knowledge of domestic violence than other social service workers, they had insufficient knowledge in communicating the risks for lethality to clients (Button & Payne, 2009). Additionally, training on domestic violence for other sectors who encounter children (i.e., healthcare, education) is critical to identifying children who may be at-risk and to increase the likelihood of a coordinated response to domestic violence (Sillito & Salari, 2011; Wathen & MacMillian, 2013).
A systematic review of training interventions on domestic violence and abuse for professionals found that programs seeking to improve the professional response to domestic violence does improve their knowledge, attitudes, competencies, and screening practice (Turner et al., 2015). Key components of these training programs include post-training discussions, “booster” sessions after training is completed, access to local domestic violence agencies, and a clear protocol for intervention. Professionals need on-going training that provides clear direction on assessing risk and that informs clinical decision making when addressing each case.
Risk Assessment. There is a lack of risk assessment tools that specifically address child risk of lethality in the context of domestic violence (Olszowy et al., 2013). It is evident from the literature that two possible options are available to solve this issue. First, a risk assessment tool specifically for a child’s risk of lethality could be developed, evaluated for reliability and validity, and standardized. Second, research indicates that standardized risk assessment tools for victims are effective in determining the level of a child’s risk, based on the notion that when a mother is at-risk then her children are also at-risk (Olszowy et al., 2013). Both possibilities require further investigation into their utility and application in various contexts and populations and where collaboration of multiple professionals in different sectors is required.
Safety Planning. The literature on safety planning in the context of domestic violence for victims and their children highlights many key components to ensuring the safety of all involved (Horton et al., 2014). Separation may not be an effective safety plan as it is a period of increased risk (Hamilton et al., 2013; Horton et al., 2014). Victims and their families require more pragmatic solutions including (a) connecting the family with relevant community services (e.g., safe housing), (b) providing financial assistance for women with children in these situations to increase family stability and safety to children, (c) working with the victim to ensure safety plans that are implemented at the child’s school or daycare, and (d) creating and maintaining developmentally appropriate safety plans with children (Chanmugam & Hall, 2012; Edleson et al., 2003; Horton et al., 2014; Johnston, 2006; Kress et al., 2012; MacMillan et al., 2013).
Several studies articulate the need for flexible, ongoing, and individualized safety planning (Chanmugam & Hall, 2012; Horton et al., 2014; Jenney, 2011). Given the complex nature of domestic violence, professionals must seek adaptive and dynamic models for intervention that considers victim’s history and current self-report (Horton et al., 2014; Jenney, 2011). Professionals must recognize the complex nature of working with families where there is domestic violence and be able to work collaboratively with them while balancing victim autonomy and safety (Horton et al., 2014). Recognizing that ending a relationship can heighten the risk, it is important to review safety planning when events might represent the end of a relationship long after physical separation has occurred, such as a final divorce hearing, engaging in a new relationship, or a final child custody order. Moreover, professionals need to add child specific questions to the safety planning process (Chanmugam & Hall, 2012; Horton et al., 2014).
In the context of separation and divorce, Hardesty and Chung (2006) recommend that custody and access only be granted when appropriate safety provisions for the child and mother are in place along with a court-approved parenting plan to establish and maintain boundaries (e.g., identifying the perpetrator’s behaviours or events that trigger violence with appropriate actions). Access arrangements can be designed to protect or rebuild parenting capacities and to meet the child’s developmental needs (Johnston, 2006). Case management in some cases is left to a family court judge to decide based on the evidence that might suggest limiting contact between the offending parent and the child (Horn & Groves, 2006; Johnston, 2006). Research suggests that supervised access can act as a buffer from the perpetrator while maintaining the safety of children and victims, especially when coordinated with the justice system and community agencies (Johnston, 2006; Hardesty & Chung, 2006; Stanley et al., 2011)
Risk Management. Literature suggests an overall need for the continued development of broad services for male perpetrators as well as for more specialized services that address DV dynamics. Several authors suggest a need for intervention programs that place a focus on parenting in conjunction with other programs aimed at preventing post-separation violence (Hardesty & Chung, 2006; Wendt et al., 2015). Although parent education programs that focus on DV-related issues (i.e., the effects of DV exposure on children), as well as the ongoing evaluation of such programs (Hardesty & Chung, 2006), have been suggested, literature of existing programs’ effectiveness is limited.
System Collaborations. Given that the presence of children often increases the number of agencies involved with a family, there is a need for inter-professional, cross-disciplinary collaboration in the risk assessment, risk management, and safety planning for children living in homes where there is domestic violence (Hamilton et al., 2013). The importance of inter-professional and cross-disciplinary collaboration is emphasized throughout the literature (Department of Justice Canada, 2013; Horton et al., 2014; Fleck-Henderson, 2000; Lessard et al., 2010; Mills et al., 2000; Murphy, 2010; Shlonsky & Friend, 2007; Spath, 2003; Stanley, Miller, Richardson-Foster, & Thomson, 2011; Turner et al., 2015; Wathen & MacMillan, 2013). One promising practice identified in the literature is the utilization of high-risk case coordination protocols, whereby justice partners and other professionals from multiple sectors meet to discuss individuals identified as high risk with the goal of coordinating risk management strategies (Department of Justice Canada, 2013). Many authors have highlighted the critical nature of developing effective multi-agency structures that focus on engaging a range of agencies (i.e., addictions and mental health, PAR programs, shelters, and victim advocates) in delivering services to perpetrators (Kohl et al., 2005; Stanley et al., 2010; Murphy, 2010) and becoming more collaborative in approaches toward risk management (Lessard et al., 2010). This type of case planning can focus on the safety and well-being of all victims within the family.
While much of the literature advocates for collaboration between professionals, there are barriers that must be addressed to do this more effectively (Department of Justice Canada, 2013; Stanley & Humphreys, 2014). Research on collaboration between police and social services in the U.K. indicates informational discrepancies in 40% of cases, along with limited ongoing communication, when comparing police reports and social work case records (Stanley et al., 2011). Some authors have recommended that professionals need to spend time together working on joint tasks to understand the nature of the differences experienced between sectors (Stanley et al., 2014).
Issues in cross-sector collaboration often originate in concerns regarding information sharing and confidentiality (Kress et al., 2012; Stanley & Humphreys, 2014). Policies and practices must be developed between sectors to address this issue in a manner that does not inhibit risk assessment efforts. One suggestion toward effective multi-agency risk assessments is developing a common assessment tool to communicate risk across disciplines and with the client (Stanley & Humphreys, 2014).
System responses to domestic violence can be fragmented due to opposing interests and mandates (Jaffe, Campbell, Olszowy, & Hamilton, 2014; Jaffe et al., 2015; Murphy, 2010; Turner et al., 2015). Moreover, professionals across various sectors may differ in their recognition of DV indicators. Research on this subject has demonstrated low concordance among professionals in different sectors (e.g., child protection, police, or lawyers) on past or current indicators of DV in cases that occurred with child maltreatment (Spath, 2003). The role of judicial education and coordinating efforts of the criminal and family courts has also been deemed to be essential (Martinson & Jackson, 2017).
Failing to effectively communicate information related to risk and failing to coordinate services to the family can be fatal (Department of Justice, 2013; Jaffe et al., 2012, 2014). In domestic violence cases, children are often overlooked as being at-risk for lethal violence and may be missed when it comes to safety planning and risk management (Hamilton et al., 2013; Jaffe et al., 2014). Additionally, when the child protection system is involved with safety planning, an adult victim may be pressured to separate from the abuser, without carefully considering the impact of the risk posed by that separation (Jaffe et al., 2012). In some circumstances, separation may result in the end of violence for women and children, but it is also a factor frequently cited in death reviews as increasing risk of lethality for the victim (Brown & Tyson, 2012; Jaffe & Juodis, 2006). Moreover, it has been found that intervention with social services often ceases once separation has occurred, despite knowing that it is a heightened period of risk (Stanley et al., 2010). This highlights the importance of understanding how risk factors need to be addressed in safety planning and risk management.
An Intersectional Review with the Vulnerable Populations
Authors: Nicole Jeffrey, Myrna Dawson
Contributors: Marcie Campbell, Jordan Fairbairn
An intersectional approach challenges a monolithic understanding of domestic violence and is, therefore, essential for understanding and addressing domestic violence among diverse populations. Whereas most domestic violence research treats categories such as gender, race, and class as separate (and often as control variables to be removed), an intersectional approach understands them as interconnected and having important compounding effects on experience. This approach also understands such categories or social identities/locations as “situated within a context of privilege and oppression rather than […] simply as demographic characteristics” (Etherington & Baker, 2016, p. 12). The intersections of various social identities/locations can influence many factors including: (a) how domestic violence is experienced and interpreted by women and responded to by others; barriers to obtaining support and safety; personal and social consequences; and if and how support and services help victims and perpetrators (Adams & Campbell, 2012; Bograd, 1999; Brassard et al., 2015; Sandberg, 2013; Sokoloff, 2008a, 2008b).
While our above reviews of the four populations separately highlight the risk factors and vulnerabilities related to domestic violence and homicide for each, we turn now to research that examines the intersections of these groups. To date, an intersectional approach has been used in domestic violence research and theory development with each of the four vulnerable populations. Some of this work has used an intersectional framework explicitly, and some has simply examined domestic violence and homicide among groups which exist across multiple social identities/locations (e.g., Indigenous populations living in rural, remote, or Northern locations). This is termed “implicit intersectional analyses” (Lykke, 2010, p. 76).
Immigrants and Refugees
Intersectional research and practice among immigrant and refugee populations stress that (a) traditional understandings of domestic violence (based largely on the experiences of White, middle class, western women) may not fit the experiences of immigrants and refugees and (b) there is significant diversity among immigrants and refugees (Sokoloff, 2008). Instead of universalizing, intersectional research accounts for how hierarchies of race, class, gender, ethnicity, nationality, and immigrant status interact to differentially impact domestic violence experiences and responses (Adams & Campbell, 2012; Erez et al., 2009; Lee & Hadeed, 2009; Sokoloff, 2008). In so doing, this work also emphasizes the need for understanding how (a) the complexity of both immigrant and host culture, including cultural differences based on “generation, geographic concentration, country of origin, [and] diasporic [migration] influences”; and (b) both contemporary and historical conditions (e.g., colonization or slavery) might differentially impact domestic violence experiences (Rees & Pease, 2007; Sokoloff, 2008, p. 235; Vaughan et al., 2015).
Research finds that intersecting social identities/locations such as gender, ethnicity, and immigration and legal status influence immigrant and refugee women’s domestic violence experiences and barriers to help-seeking by contributing to (a) limited access or awareness of services; (b) legal dependency on their abusers; (c) fear of losing the support of their immigrant communities; (d) isolation; (e) fear of deportation; (f) financial, educational, and occupational constraints; (g) acculturation stress; (h) traditional gender and marital roles; and (i) language barriers (Adams & Campbell, 2012; Bhuyan & Velagapudi, 2013; Erez et al., 2009; Lee & Hadeed, 2009; Liao, 2006; Rees & Pease, 2007; Sokoloff, 2008; Vidales, 2010). Different immigrant and refugee groups also experience varying levels and forms of bias and discrimination by the general public, healthcare and criminal justice professionals, and other service providers (Erez et al., 2009; Humphreys, Sharps, & Campbell, 2005; Liao, 2006), all of which might impact their experiences of domestic violence and help seeking.
Indigenous Populations
Applied to Indigenous populations, an intersectional approach highlights the impact of the intersections of gender, cultural heritage, physical ability, social class, geography (rural/urban), and other factors—and, thus, various systems of oppression such as colonialism, patriarchy, racism, and capitalism—on Indigenous women’s domestic violence experiences (Australia’s National Research Organisation for Women’s Safety [ANROWS], 2015a; Brassard et al., 2015; Centre de recherché interdisciplinaire sur la violence familiale et la violence faite aux femmes [CRI-VIFF], 2011; Shepherd, 2001). Such intersections may shape Indigenous women’s exposure to domestic violence, how they make sense of such violence, and their ability to find safety (CRI-VIFF, 2011). For example, the history of colonialism, violent assimilation practices, residential schools, large-scale apprehension of Indigenous children by child protection services, and forced relocation has triggered generational trauma, normalization and reproduction of violence, and disruption of families, relationships, and traditions (Campbell, 2007; CRI-VIFF, 2011; Brassard et al., 2015). Moreover, Indigenous communities experience continued discrimination, limited employment opportunities, poor living conditions, and limited social resources (ANROWS, 2015a; CRI-VIFF, 2011); all of these factors can interact with other social identities/locations to impact domestic violence experiences.
Rural, Remote, and Northern Populations
Rural/urban geographies have seldom been included in explicitly intersectional analyses of domestic violence. Sandberg (2013) argues that this is an important gap in the literature, stating that rurality can “impose particular kinds of vulnerability to individuals” (Sandberg, 2013, p. 361). Such vulnerabilities include physical and social isolation; harsh weather conditions; poverty; lack of transportation or jobs; lack of resources and information related to DV; and anonymity and confidentiality. An intersectional framework examines how these vulnerabilities interact with other social identities/locations—such as race, ethnicity, disability, immigrant status, and Indigeneity—to impact rural, remote, and northern women’s domestic violence experiences and help-seeking (Grossman, Hinkley, Kawalski, & Margrave, 2005; Sandberg, 2013; Shepherd, 2001). For example, one study found that Black rural victims (compared to Black urban victims, White rural victims, and urban White victims) were in need of transportation, suggesting barriers to this resource related to both race and rurality (Grossman et al., 2005). As with immigrant and refugee populations, researchers applying intersectionality to rural, remote, and northern populations stress that not all such populations are the same and that this contextual variability should be examined (Sandberg, 2013).
Indigenous Rural, Remote, and Northern Populations
Although not always explicitly intersectional, considerable research has examined the compounding vulnerabilities for Indigenous populations living in rural, remote, or northern areas (e.g., Brassard et al., 2015; Campbell, 2007; Gordon et al., 2002; Shepherd, 2001). This vulnerability is most evident in domestic violence prevalence rates; Indigenous women living in rural and remote areas are one and a half times more likely to experience domestic violence than those living in metropolitan areas and 45 times more likely than the non-Indigenous population (Ferrante, Morgan, Indermaur, & Harding, 1996). Many of the issues faced by Indigenous populations overlap with and are intensified by those faced in rural, remote, or Northern regions—such as social and physical isolation, lack of accessible and culturally-appropriate services, limited employment options, limited transportation, housing issues, social pressures to remain silent about abuse, and prevalence of alcohol and firearms (Bagshaw, Chung, Couch, Lilburn, & Wadham, 2000; Brassard et al., 2015; Gordon et al., 2002; Shepherd, 2001). The combination of these vulnerabilities puts DV victims in danger and may account for the high frequency and severity of domestic violence and homicide among rural Indigenous women (Bagshaw et al., 2000; Brassard et al., 2015; Gordon et al., 2002; Shepherd, 2001).
Barriers to leaving an abuser are also compounded among rural, remote, and northern Indigenous victims because many do not want to leave the community (which is the home of family, friends, and traditions); services may not be available in their Indigenous language; shelter and other service employees may not understand and respect their cultural values; travelling can be expensive or unfeasible; the location of shelters may not be private; and geographic isolation may reinforce the isolation and control that abusers impose on victims (Brassard et al., 2015; Campbell, 2007, p. 71; Gordon, Hallahan, & Henry, 2002; Shepherd, 2001).
Immigrant Rural, Remote, and Northern Populations
Some research has also examined the compounding vulnerabilities for immigrant populations living in rural, remote, or northern areas. Most notably, this work has highlighted that the combination of these social identities/locations may exacerbate social isolation (Denham et al., 2007). For example, often immigrants in rural areas do not have a strong community to turn to for support because there are few other immigrants in the area (Denham et al., 2007). Moreover, rural communities are often ill prepared to offer culturally and linguistically appropriate services (Denham et al., 2007; Hancock, 2006). This lack of social networks due to geographic isolation has been empirically linked to greater likelihood of domestic violence for immigrant women from developed countries (Brownridge & Halli, 2002). Other work has discussed the role of machismo and corresponding rigid female gender roles in domestic violence among Latino immigrants and that such roles are even more extreme in rural settings, which tend to adhere to traditional and patriarchal values (Welland & Ribner, 2010).
Children Exposed to Domestic Violence
Research and practice with children exposed to domestic violence has seldom used an explicitly intersectional framework. Nevertheless, it is important to recognize how social identities/locations and layers of oppression related to race, gender, class, immigrant status, Indigeneity, geography, and so on—in addition to age and developmental level—can impact children’s experiences of domestic violence. Etherington and Baker (2016) argue that intersectional approaches with children must understand that children have their own identities and social categories, separate from those of their families, that will differentially impact their experiences. For example, a second-generation immigrant child’s experiences may be different from those of their first-generation parents. Where possible, researchers should also consider children’s own understandings of their identities (Etherington & Baker, 2016). As with victims of domestic violence, the intersections of children’s social identities/locations might influence exposure to domestic violence; perceptions of and responses to domestic violence; and help-seeking, coping, and adjustment following exposure (Etherington & Baker, 2016; Kennedy, Bybee, Kulkarni, & Archer, 2013; Tailor & Letourneau, 2012).
Highlighting the impact of intersecting social identities/locations, research has found that low-income rural families have a heightened risk of domestic violence, especially around the birth of a child (and that this risk decreases over the first 5 years of a child’s life; Gustafsson et al., 2016). In some cases of what is often called “honour-based violence” among immigrant communities, children have been killed both accidentally and intentionally in attacks; for example, if relatives or spouses “believe the children have been tainted by their mother’s supposed immorality” (Brandon & Hafez, 2008, p. 51). Finally, children with immigrant parents are at increased risk of being exposed to domestic violence, likely due to the increased vulnerabilities experienced in immigrant populations (Bø Vatnar & Bjørkly, 2010; see Table 3 in Discussion chapter).
Intersectional Policy and Practice
Although to-date intersectional research on domestic violence risk assessment, risk management, and safety planning strategies has been limited, there are some preliminary ideas for intersectional policy and practice that can be developed from existing literature. Domestic violence prevalence data suggest that certain populations experiencing multiple, intersecting axes of oppression could be targeted for screening and intervention (e.g., low-income rural families, especially around the birth of a new child; Gustafsson et al., 2016). However, as highlighted by an intersectional approach, such screening and intervention should (a) be comprehensive and consider the lived experiences of diverse populations, (b) be culturally-appropriate, (c) address the social and structural conditions of these populations, and (d) include multi-sector collaboration.
With respect to policy and practice, an intersectional approach emphasizes the importance both of questioning assumptions that victims exist only within dominant groups (e.g., White, middle class, and able-bodied) and also of identifying solutions for addressing barriers (e.g., accessing services) for different populations (Etherington & Baker, 2016). Indeed, addressing domestic violence is complex because “depending on the context and circumstances, a resource for [some populations] could equally represent a barrier” for others (Bhuyan & Velagapudi, 2013, p. 70). For example, turning to the police or applying for social assistance (important resources for many victims) can result in deportation of undocumented immigrant victims or their abusers if authorities report them (Bhuyan & Velagapudi, 2013). Thus, intersectional policy and practice is “not about designing one policy or program for every specific combination of identities but rather taking a comprehensive approach to the problem” of domestic violence so that the experiences of diverse populations are considered (Etherington & Baker, 2016, p. 13). Many women’s shelters, for example, have been influenced by feminist intersectional perspectives and are moving away from homogenizing approaches to domestic violence (Australia’s National Research Organisation for Women’s Safety [ANROWS], 2015b). Intersectional perspectives allow shelters to provide more inclusive responses to particular groups of women, such as women with disabilities and Indigenous women (ANROWS, 2015b).
Inclusive, culturally-appropriate services should be available for diverse populations and should consider the intersecting social identities/locations noted above. For example, shelters might employ Indigenous Liaison Officers to “help build relationships and a rapport with local Indigenous communities” or might be specifically devoted to supporting Indigenous women (ANROWS, 2015, p. 21). Child welfare practices among Indigenous children exposed to family violence should consider the long-term risks and consequences of separating children from their family, culture, identity, and community (even in cases where there might be short-term risk aversion by removing the child from the home; Riggs, 2015). This is especially important given that Indigenous children are overrepresented in the child protection system and that apprehension might be experienced as racism (NSW Department of Health, 2011; Riggs, 2015). They should also provide opportunities to engage in cultural ceremonies, connections with Elders, cultural support services, and so on (Riggs, 2015). Nixon, Bonnycastle, and Ens (2015) suggest that professionals should be aware of northern Indigenous mothers’ reliance on informal supports such as family, friends, and community members—likely related to traditional Indigenous values, the scarcity of formal resources available, and mistrust of helping professionals—and challenge notions of these mothers’ failure to protect their children. Focusing on these mothers’ strengths and protective capacities may also help “limit unnecessary, inappropriate, or intrusive [child protection] interventions” (Nixon et al., 2015, p. 1). The centrality of tight-knit families in Indigenous communities also means that children (and other family members) may be more heavily impacted by witnessing domestic violence and that interventions must, therefore, span multiple levels and generations (Burnette & Cannon, 2014).
In addition to culturally-appropriate services, an intersectional approach encourages strategies that address the social and structural conditions such as poverty and poor housing; these can exacerbate vulnerability to domestic violence and subsequent outcomes (Etherington & Baker, 2016; Gordon et al., 2002; Sokoloff, 2008). For example, social workers and others seeking to support rural, remote, and northern victims might consider strategies to address the simultaneous isolation and lack of anonymity experienced by many (Sandberg, 2013). Providing affordable housing to rural and remote Indigenous women who otherwise often face homelessness or overcrowding may help to address domestic violence (Gordon et al., 2002). In addition to being culturally-trained, service providers should be able to travel or provide outreach services to Indigenous communities living in rural, remote, or northern regions (Bagshaw et al., 2000; Victorian Indigenous Family Violence Task Force, 2003). The additional isolation that immigrant victims living in rural, remote, or northern areas experience suggests that social service providers should help women build social support networks; for example, they could bring Latina or other immigrant women together to provide emotional support to each other or help them to establish connections with distant family members (Denham et al., 2007; Hancock, 2006; Hancock & Ames, 2008).
Finally, multi-sector collaboration and coordination have been widely recommended to help address diverse vulnerabilities. Coordinated and collaborative responses may be particularly helpful for rural, remote, and northern Indigenous communities because they offer financial savings, consistent response, and effective use of resources; they also allow locally-focused and culturally-appropriate service provision (Gordon et al., 2002). Nevertheless, collaborative responses have also been recommended for addressing the multiple identities and oppressions that impact children’s exposure to domestic violence (Etherington & Baker, 2016) and for providing a more effective way of reaching and helping immigrants living in rural, remote, and northern areas (e.g., social workers might collaborate with Latino church leaders; Hancock, 2006; Hancock & Ames, 2008).
Although still very much in early stages, intersectional domestic violence research and practices underscore the importance of attending to intersecting categories for both understanding and addressing domestic violence among diverse and vulnerable populations. We have included some research in this section that has not explicitly used an intersectional framework but has nevertheless examined domestic violence and homicide among groups who exist across multiple social identities/locations. However, some argue that effective intersectionality research must intentionally ground itself in an intersectional framework and incorporate it throughout every stage of the research (Etherington & Baker, 2016; Norris, Zajicek, & Murphy-Erby, 2010). Thus, domestic violence research among vulnerable populations should continue to move beyond treating different social identities/locations as demographic variables and instead focus more deeply on the structural inequalities related to such identities/locations and the compounding effects they have on experience.
Discussion
Authors: Nicole Jeffrey, Myrna Dawson
Contributors: Wendy Verhoek-Oftedahl, Marcie Campbell, Peter Jaffe
Domestic violence and homicide are serious and pervasive public health issues in Canada and worldwide (Campbell et al., 2003; Johnson & Dawson, 2011; Public Health Agency of Canada, 2016; World Health Organization, 2012). This literature review has focused on four populations: (1) Indigenous populations, (2) immigrant and refugee populations, (3) rural, remote, and northern populations, and (4) children exposed to domestic violence. Each experience factors that increase their vulnerability to domestic violence and homicide; influence their victimization experiences; exacerbate their negative mental and physical health outcomes; and hinder their ability and willingness to report abuse, obtain support and services, and find safety.
Despite mounting evidence for these vulnerabilities, most research and practice continue to use a one-size-fits-all approach to understanding and addressing domestic violence and homicide. This literature review offers a first preliminary step towards moving beyond this traditional approach to consider and synthesize different and intersecting challenges and experiences among the four populations. Table 3 summarizes our review findings regarding vulnerabilities, risk assessment, risk management, and safety planning among the four populations. The vulnerabilities and prevention strategies are a combination of individual, relational, community, and societal factors that contribute to the risk and that identify the multiple levels for prevention.
Table 3: Summary of Vulnerabilities and Findings Regarding Risk Assessment, Risk Management, and Safety Planning Across the Four Vulnerable Populations
|
Population |
Vulnerabilities |
Risk Assessment |
Risk Management |
Safety Planning |
|
Indigenous |
|
|
|
|
|
Rural, Remote, & Northern (RRN) |
|
|
|
|
|
Immigrant & Refugee (IR) |
|
|
|
|
|
Children Experiencing Domestic Violence |
|
|
|
|
The Need for Differentiated, Social, and Intersectional Approaches
Many of the risk factors and recommendations for risk assessment, risk management, and safety planning overlap between the four vulnerable populations (as can be seen in Table 3). For example, most of the groups experience economic and structural issues (e.g., poverty and lack of housing and employment opportunities), isolation, traditional patriarchal values and cultural norms conducive to domestic violence, as well as limited access to services and resources. Nevertheless, a key take-away from this review is that these factors can impact domestic violence experiences in different ways across the four groups, thus supporting the need for differentiated approaches to understanding and addressing domestic violence and homicide. This includes culturally-appropriate or context-specific services, risk assessment, risk management, and safety planning. Considering that much of the literature and our review has grouped vulnerable populations into single categories and also that some risk factors and conditions may be common within these populations, context-specific approaches should recognize the variability within Indigenous, RRN, Immigrant and Refugee, and child populations, respectively (Burnman et al., 2004; Raj & Silverman, 2002).
As discussed at the outset of this report, social ecological and intersectional frameworks may be particularly useful in identifying valid differentiated approaches and in understanding the different and overlapping characteristics and conditions that impact domestic violence experiences. Together, these two frameworks suggest that risk assessment, risk management, and safety planning strategies work at multiple levels and that they consider intersecting axes of oppression and sociocultural/historical aspects of risk and experience. This is important given that there is no single explanatory factor to explain why violence and contributors exist at various levels. As such, the social ecological approach focuses not only on the individual level but also on relationship, community, and societal levels. Understanding and addressing victims’ “entire ecological context” is especially important among vulnerable and marginalized populations (Nelson & Lund, 2017) because the traditional focus on individual-level risk factors (Cunradi, 2010) is particularly problematic among vulnerable populations who often experience additional social and structural risk factors and barriers. Indeed, our review highlights the strength and degree of social factors in impacting domestic violence and homicide among the four vulnerable populations. For example, colonization, poverty, isolation, traditional norms, limited employment opportunities, and other social factors can greatly impact women’s vulnerability to domestic violence and homicide and their ability and willingness to seek support. Strategies to address risk and safety must take these levels into account (Hyman et al., 2011). Moreover, a focus on the individual may be inappropriate in some groups; for example, Indigenous populations emphasize the role of the whole community in the experience and prevention of violence.
An intersectional framework also challenges one-size-fits-all approaches to domestic violence by considering how various social identities intersect to shape experience (Crenshaw, 1989, 1991; Erez et al., 2009). Recognizing intersectionality is key for understanding the structural and cultural dimensions of domestic violence (Sokoloff, 2008a). As demonstrated above, intersectionality can provide a more nuanced understanding of the needs and experiences of diverse populations, which can, in turn, assist in the creation of more relevant, effective, and culturally-sensitive services and policies. Indeed, strategies that are developed based on the experiences of just one group of women or that overlook how additional axes of oppression shape some women’s lives will be less fruitful for (and potentially harmful to) some other groups of women (Crenshaw, 1991; Sokoloff & Dupont, 2005). This may be particularly important in the areas of risk assessment, risk management, and safety planning.
Some researchers have explicitly combined intersectional and social ecological approaches in examining the conditions of vulnerable populations, including domestic violence (e.g., Guruge & Khanlou, 2004; Vaughan et al., 2015). However, they seem to define race, class, gender, and other identities at the individual level—in contrast to the conceptualization of these dimensions as social locations and/or identities in most intersectional frameworks described above. Nevertheless, used together, the two frameworks “[provide] a basis for analysis of the complex issues at the intersection of race, gender, and class identities (both imposed and assumed) and the interaction of these and other identities” with factors and issues at the familial, community, and sociocultural levels (Guruge & Khanlou, 2004, p. 38).
This review has also been guided by the principles of exposure reduction. However, on its own, this theoretical lens may be insufficient for understanding and addressing domestic violence and homicide, especially among vulnerable populations. For example, safety planning and risk management strategies that focus on reducing exposure between victims and perpetrators by encouraging women to leave an abusive partner may be inappropriate in some populations. Each of the four vulnerable populations experience many barriers to leaving an abusive partner including: (a) geographic and social isolation; (b) long-established ties to family, the community, and property; (c) traditional values around keeping the family together; (d) economic dependence on the abuser and/or lack of employment opportunities; and € custody conflicts and other issues related to access to children (Brassard et al., 2015; Denham et al., 2007; Doherty & Hornosty, 2004; Lessard et al., 2010; Social Development Committee of the Parliament of South Australia, 2016). Because leaving an abuser is not always a viable or safe option, our review suggests that risk management and safety planning should move beyond traditional exposure-reducing strategies. These might include, for example, providing strategies to minimize harm (e.g., have perpetrators attend an intervention for fathers such as Caring Dads https://www.caringdads.org/) and having child protection workers work directly with domestic violence perpetrators (Doherty & Hornosty, 2004; Jenney, 2011; Midlarsky et al., 2006). When exposure reduction is the goal, risk management and safety planning should at a minimum consider the different needs of each population at multiple levels, including the impact of intersecting axes of oppression (e.g., enhanced social isolation among immigrant populations living in rural, remote, or northern areas; Denham et al., 2007).
Priorities for Future Research and Practice
While our review turned up hundreds of works on domestic violence or homicide in one or more of the four vulnerable populations, more work is still needed. Several key priorities have been reiterated in the literature across all the four vulnerable populations. In each of the sections below, we offer a list of key recommendations and priorities identified in the literature for improving and expanding future domestic violence research and practice.
Research
- Empirical or more evidence-based examinations and comparisons of vulnerabilities and risk factors (e.g., rural compared to nonrural, immigrant compared to non-immigrant)
- Development and evaluation of population-specific, culturally-informed risk assessment tools, risk management and safety planning strategies, and other services and supports
- Research that extends beyond the individual and relational correlates of domestic violence and examines community, social, cultural, and historical context
- Intersectional research among diverse vulnerable populations (e.g., RRN women with disabilities, Indigenous and immigrant populations living in RRN areas)
Practice
- Development and implementation of population-specific, culturally-informed risk assessment tools or guidelines to enhance existing tools, risk management and safety planning strategies by using a special lens to consider risk in different vulnerable populations
- Increased funding and resources to address the scarcity of resources and services in many communities
- Expanded and improved training and education (on domestic violence and cultural competence) for service providers working with vulnerable populations
- Implementation of strategies and supports that address community, social, cultural, historical, and structural inequalities
- Implementation of efforts to reduce barriers and increase access to services and resources
- Development and implementation of service/sector coordination and collaboration
Summary and Conclusions
Authors: Marcie Campbell, Peter Jaffe, Myrna Dawson
Contributors: Jordan Fairbairn
This literature review was undertaken as part of a SSHRC-funded initiative focused on preventing domestic homicides in vulnerable populations. Although there are multiple groups or populations that are considered vulnerable in the context of domestic violence, this review focused on four specific populations based on the current literature: (1) Indigenous populations, (2) immigrant and refugee populations, (3) rural, remote, and northern populations, and (4) children exposed to domestic violence. However, it is recognized that these are not mutually exclusive groups given that individuals may be members in intersecting and overlapping groups.
This literature review highlights not only the increased risk for homicide with these populations but also the specific factors that increase their vulnerability. The literature is consistent in demonstrating the challenges these groups face around reporting violence and abuse, obtaining support and services, and finding safety.
Current research and practice tends to take a traditional and general approach to understanding and addressing domestic violence and homicide. This literature review offers a first preliminary step towards moving beyond this standard approach to consider and synthesize specific and intersecting challenges and experiences among the four populations.
The social ecological and intersectional frameworks suggest that risk assessment, risk management, and safety planning strategies work at multiple levels and consider intersecting axes of oppression and sociocultural/historical aspects of risk and experience. The social ecological approach focuses not only on the individual level but also on relationship, community, and societal levels. Understanding and addressing victims’ ecological context is especially important among vulnerable and marginalized populations who often experience additional social and structural risks and barriers. This literature review highlights the strength and degree of social factors in impacting domestic violence and homicide among the four vulnerable populations. An intersectional framework also challenges the generic approach to addressing domestic violence and homicide by considering how various social identities and locations intersect to shape experience. Recognizing that intersectionality is key for understanding the structural and cultural dimensions of domestic violence and intersectionality can provide a more nuanced understanding of the needs and experiences of diverse populations to help create more relevant, effective, and culturally-sensitive services and policies around risk assessment, risk management, and safety planning.
This review has also been guided by the principles of exposure reduction; however, this lens may not be sufficient for understanding and addressing domestic violence and homicide particularly among the vulnerable populations. Safety planning and risk management strategies that focus on reducing exposure between victims/survivors and perpetrators may not always be conducive when there are challenges and barriers associated with geographic location, community and family, economics, values, and custody/access of children. This literature review suggests that risk management and safety planning should move beyond traditional exposure-reducing strategies; and it also suggests that when exposure reduction is the goal then risk management and safety planning should at a minimum consider the needs of each population at multiple levels, including the impact of intersecting axes of oppression.
This literature review reveals that more research is still needed regarding preventing domestic homicide within vulnerable populations. There needs to be more empirical research on specific vulnerabilities and risks for these populations to help inform the development and evaluation of population-specific, culturally-informed risk assessment tools, risk management, and safety planning strategies. Most important, there is a need for more intersectional research on addressing domestic violence and homicide among diverse vulnerable populations.
Finally, this literature review helps to inform priorities for future practice and policy. These priorities include developing and implementing population-specific, culturally-informed risk assessment tools or guidelines as well as risk management and safety planning strategies; increasing and enhancing training and education for service providers working with vulnerable populations; and implementing strategies and supports that address inequalities, reduce barriers, and increase access to resources and services.
The tag line that domestic violence affects everyone equally trivializes both the dimensions that underlie the experiences of these particular abuse victims and more important, the ways we analyze the prevalence and impact of violence against them (Kanuha, 1996, p. 41 as cited in Sokoloff & Dupont, 2005)
References
- Abrahams, N., Mathews, S., Martin, L. J., Lombard, C., & Jewkes, R. (2013). Intimate partner femicide in South Africa in 1999 and 2009. PLoS Med, 10(4): e1001412. doi: 10.1371/journal.pmed.1001412
- Abu-Ras, W. (2007). Cultural beliefs and service utilization by battered Arab immigrant women. Violence Against Women, 13(10), 1002-1028. doi: 10.1177/1077801207306019
- Acevedo, M. J. (2000). Battered immigrant Mexican women's perspectives regarding abuse and help-seeking. Journal of Multicultural Social Work, 8(3-4), 243-282. doi: 10.1300/J285v08n03_04
- Adam, N. M. (2000). Domestic violence against women within immigrant Indian and Pakistani communities in the United States (Doctoral dissertation). Retrieved from ProQuest Dissertations and Theses database. (UMI No. 9993857)
- Adams, M. E., & Campbell, J. (2012). Being undocumented & intimate partner violence (IPV): Multiple vulnerabilities through the lens of feminist intersectionality. Women’s Health & Urban Life, 11, 15-34. Retrieved fromhttps://tspace.library.utoronto.ca/bitstream/1807/32411/1/11.1_Adams_%26...
- Ahmadzai, M. (2015). A study on visible minority immigrant women's experiences with domestic violence. Social Justice and Community Engagement. 14. Retrieved from http://scholars.wlu.ca/cgi/viewcontent.cgi?article=1014&context=brantford_sjce
- Alaggia, R., Regehr, C., & Jenney, A., 2012. Risky business: An ecological analysis of intimate partner violence disclosure. Research on Social Work Practice, 22(3), pp.301-312. doi: 10.1177/1049731511425503
- Alberta Council of Women’s Shelters & Campbell, J. (2014). Walking the path together tools: Danger Assessment phase II. Retrieved from Alberta Council of Women’s Shelters website: https://www.acws.ca/collaborate-document/2516/view
- Alberta Family Violence Death Review Committee. (2015). Annual report to the Minister of Human Services. Retrieved from http://www.humanservices.alberta.ca/ documents/family-violence-death-review-annual-report-2014-15.pdf
- Aldridge, M. L., & Browne, K. D. (2003). Perpetrators of spousal homicide: A review. Trauma, Violence, & Abuse, 4(3), 265-276. doi: 10.1177/1524838003253875
- Allan, A., & Dawson, D. (2002). Developing a unique risk of violence tool for Australian Indigenous offenders. Retrieved from http://crg.aic.gov.au/reports/200001-06.html
- Al-Yaman, F., Doeland, M. V., & Wallis, M. (2006). Family violence among Aboriginal and Torres Strait Islander peoples. Canberra, Australia: Australian Institute of Health and Welfare. Retrieved from http://www.aihw.gov.au/publication-detail/?id=6442467912
- Amanor-Boadu, Y. (2009). A comparison of immigrant and non-immigrant women's decision making in abusive relationship (Doctoral dissertation). Retrieved from K-State Electronic Theses, Dissertations, and Report: 2004. (UMI No. 0628)
- Amanor-Boadu, Y., Messing, J. T., Stith, S. M., Anderson, J. R., O'Sullivan, C., & Campbell, J. (2012). Immigrant and non-immigrant women: Factors that predict leaving an abusive relationship. Violence and Victims, 18(5), 610-632. doi: 10.1177/1077801212453139
- Amellal, D. (2005). The “In Search of Your Warrior” program: Identity at the heart of healing. Let’s Talk, 30(4), 4-7. Retrieved from http://www.csc-scc.gc.ca/text/pblct/lt-en/2005/30-4/3-eng.shtml
- Anderson, K. M., Renner, L. M., & Bloom, T. S. (2014). Rural women’s strategic responses to intimate partner violence. Health Care for Women International, 35, 423-441. doi: 10.1080/07399332.2013.815757
- Annan, S. L. (2008). Intimate partner violence in rural environments. In A. Graubard, & J. Rosen. Annual Review of Nursing Research, 26, 85-113. New York, NY: Spring Publishing Company
- Asawa, L. E. (2008). Reducing the risk of child maltreatment through the Early Head Start program (Doctoral dissertation). Retrieved from ProQuest Dissertation & Theses Global. (UMI No. 3303505).
- Assembly of First Nations. (2013). A national action plan to end violence against Indigenous women and girls. Retrieved from http://www.afn.ca/uploads/files/aga2013/nap-endviolence.pdf
- AuCoin, K. (2005). Children and youth as victims of violent crime. Juristat. Statistics Canada Catalogue no. 85- 002-X. Retrieved from http://www.statcan.gc.ca/pub/85-002-x/85-002-x2005001-eng.pdf Augusta-Scott, T., Scott, K., & Tutty, L. M. (Eds.). (2017). Innovations in interventions to address intimate partner violence: Research and practice. New York, NY: Taylor & Francis.
- Aujla, W., & Gill, A. K. (2014). Conceptualizing 'Honour' Killings in Canada: An extreme form of domestic violence? International Journal of Criminal Justice Sciences, 9(1), 153. Retrieved from http://citeseerx.ist.psu.edu/viewdoc/download;jsessionid=A08966C70E32AE0...
- Australia’s National Research Organisation for Women’s Safety. (2015a). Innovative models in addressing violence against Indigenous women: State of knowledge paper. Retrieved from https://anrows.org.au/publications/landscapes-0/innovative-models-in-add...
- Australia’s National Research Organisation for Women’s Safety. (2015b). Seeking help for domestic violence: Exploring rural women’s coping experiences: State of knowledge paper. Retrieved from https://anrows.org.au/sites/default/files/4_1%203%20LandscapesRuralWomen...
- Averill, J. B., Padilla, A. O., & Clements, P. T. (2007). Frightened in isolation: Unique considerations for research of sexual assault and interpersonal violence in rural areas. Journal of Forensic Nursing, 3, 42-46. Retrieved from http://onlinelibrary.wiley.com/doi/10.1111/j.1939-3938.2007.tb00091.x/epdf
- Babcock, J. C., Green, C. E., & Robie, C. (2004). Does batterers’ treatment work? A meta-analytic review of domestic violence treatment. Clinical Psychology Review, 23, 1023-1053. doi:10.1016/j.cpr.2002.07.001
- Bagshaw, D., Chung, D., Couch, M., Lilburn, S., & Wadham, B. (2000). Reshaping responses to domestic violence: Final report. Retrieved from http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.452.2467&rep=re...
- Bair-Merritt, M. H., Jennings, J. M., Chen, R., Burrell, L., McFarlane, E., Fuddy, L., & Duggan, A. K. (2010). Reducing maternal intimate partner violence after the birth of a child: A randomized controlled trial of the Hawaii healthy start home visitation program. Archives of Pediatrics & Adolescent Medicine, 164(1), 16. doi: 10.1001/archpediatrics.2009.237
- Baker, L. B., Jaffe, P. G., Berkowitz, S. J., & Berkman, M. (2002). Children exposed to violence: A handbook for police trainers to increase understanding and improve community responses. London, ON: Centre for Children & Families in the Justice System. Retrieved from http://www.lfcc.on.ca/police-us.PDF
- Banman, V. L. (2015). Domestic homicide risk factors: Rural and urban considerations (Unpublished master’s thesis). Thesis and Dissertation Repository. (2767). The University of Western Ontario, London, ON.
- Baobaid, M. (2012). Domestic violence risks in families with collectivist values: Understanding cultural context. Retrieved from http://onlinetraining.learningtoendabuse.ca/sites/default/files/lessons/...
- Baobaid, M. (n.d.). Outreach strategies for family violence intervention with immigrant and minority communities: Lessons learned from the Muslim Family Safety Project. Retrieved from http://www.yemenembassy.ca/doc/Outreach%20Strategies.pdf
- Baobaid, M., & Hamed, G. (2010). Addressing domestic violence in Canadian Muslim communities: A training manual for Muslim communities and Ontario service providers. Retrieved from http://www.learningtoendabuse.ca/sites/default/files/MFSP_Manual_2010.pdf
- Barton, S., Hungler, K., McBride, D., Letourneau, N., & Mailloux, S. (2015). Alberta Research Project Report for Provincial Stakeholders: Rural and Northern Community Response to Intimate Partner Violence. Retrieved from University of Alberta, Faculty of Nursing website http://www2.uregina.ca/ipv/Research%20Documents/AB%20-%20IPV%20Community...
- Battered Women's Support Services. (2010). Empowering non-status, refugee, and immigrant women who experience violence (manual). Retrieved from http://www.bwss.org/wp-content/uploads/2010/07/NSRIW-MANUAL.pdf
- Bauer, H. M., Rodriguez, M. A., Quiroga, S. S., & Flores-Ortiz, Y. G. (2000). Barriers to health care for abused Latina and Asian immigrant women. Journal of Health Care for the Poor and Underserved, 11(1), 33-44. doi: 10.1353/hpu.2010.0590
- Beaupré, P. (2015). “Family violence in Canada: A statistical profile, 2013.” Juristat. Statistics Canada Catalogue no. 85-002-X., p.1-85. Retrieved from www.statcan.gc.ca/pub/85-002-x/2014001/article/14114-eng.pdf
- Belfrage, H., Strand, S., Ekman, L., & Hasselborg, A.-K. (2012a). Assessing risk of patriarchal violence with honour as a motive: Six years’ experience using the PATRIARCH checklist. International Journal of Police Science & Management, 14(1), 20-29. doi: 10.1350/ijps.2012.14.1.250
- Belfrage, H., Strand, S., Storey, J. E., Gibas, A. L., Kropp, P. R., & Hart, S. D. (2012b). Assessment and management of risk for intimate partner violence by police officers using the Spousal Assault Risk Assessment Guide. Law and Human Behavior, 36, 60-67. doi:10.1037/h0093948
- Belknap, R. A., & Vandevusse, L. (2010). Listening sessions with Latinas: documenting life contexts and creating connections. Public Health Nursing, 27(4), 337-346. doi:10.1111/j.1525-1446.2010.00864.x
- Bender, A. (2015). Rural primary health care providers’ response to intimate partner violence and survivors’ perceptions of helpfulness (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (UMI No. 3700233). Washington State University, St. Louis, MO.
- Ben-Porat, A. (2010). Connecting two worlds: Training social workers to deal with domestic violence against women in the Ethiopian community. The British Journal of Social Work, 40(8), 2485-2501. doi: 10.1093/bjsw/bcq027
- Berry, J. W. (1997). Immigration, acculturation, and adaptation. Applied Psychology: An International Review, 46(1), 5-68. doi: 10.1111/j.1464-0597.1997.tb01087.x
- Berry, J. W. (2005). Acculturation: Living successfully in two cultures. International Journal of Intercultural Relations, 29, 697-712. doi:10.1016/j.ijintrel.2005.07.013
- Beyer, K. M., Layde, P. M., Hamberger, L. K., & Laud, P. W. (2013). Characteristics of the residential neighborhood environment differentiate intimate partner femicide in urban versus rural settings. Journal of Rural Health, 29, 281-293. doi: 10.1111/j.1748-0361.2012.00448.x
- Beyer, K., Wallis, A. B., & Hamberger, L. K. (2015). Neighbourhood environment and intimate partner violence: A systematic review. Trauma, Violence, & Abuse, 16, 16-47. doi: 10.1177/1524838013515758
- Bhandari, S., Bullock, L. F., & Sharps, P. W. (2013). Strategies pregnant rural women employ to deal with intimate partner violence. Journal of Ethnographic & Qualitative Research, 7, 143-154.
- Biesenthal, L., Sproule, L. D., Nelder, M., Golton, S., Mann, D., Podovinnikoff, D., …Lunn, D with Community Abuse Programs of Rural Ontario. (2000, July). The Ontario rural woman abuse study (ORWAS): Final report. Retrieved from Department of Justice Canada website: http://www.justice.gc.ca/eng/rp-pr/cj-jp/victim/rr00_15/rr00_15.pdf
- Black, S., Dempsey, S. H., & Davis, M. B. (2010). Practitioner-recommended policies and procedures for children exposed to domestic violence. Health Promotion Practice, 11(6), 900-907. doi: 10.1177/152483990935989
- Blagg, H., Bluett-Boyd, N., & Williams, E. (2015). Innovative models in addressing violence against Indigenous women: State of knowledge paper. University of Western Australia, Crawley, WA
- Bloom, T. L., Glass, N. E., Case, J., Wright, C., Nolte, K., & Parsons, L. (2014). Feasibility of an online safety planning intervention for rural and urban pregnant abused women. Nursing Research, 63, 243-251. doi: 10.1097/NNR.0000000000000036
- Bø Vatnar, S. K., & Bjørkly, S. (2010). An interactional perspective on the relationship of immigration to intimate partner violence in a representative sample of help-seeking women. Journal of Interpersonal Violence, 25(10), 1815-1835. doi:10.1177/0886260509354511
- Bø Vatnar, S. K., & Bjørkly, S. (2010). An interactional perspective on the relationship of immigration to intimate partner violence in a representative sample of help-seeking women. Journal of Interpersonal Violence, 25(10), 1815-1835. doi: 10.1177/0886260509354511
- Bograd, M. (1999). Strengthening domestic violence theories: Intersections of race, class, sexual orientation, and gender. Journal of Marital and Family Therapy, 25, 275-289. doi: 10.1111/j.1752-0606.1999.tb00248
- Bohn, D. K. (2003). Lifetime physical and sexual abuse, substance abuse, depression, and suicide attempts among Native American women. Issues in Mental Health Nursing, 24(3), 333-352. doi:10.1080/01612840305277
- Bonta, J., & Andrews, D.A. (2007). Risk-Need-Responsivity model for offender assessment and ehabilitation 2007-06. Ottawa, ON: Department of Public Safety. Retrieved from https://www.publicsafety.gc.ca/cnt/rsrcs/pblctns/rsk-nd-rspnsvty/rsk-nd-...
- Borowsky, I. W., & Ireland, M. (2002). Parental screening for intimate partner violence by pediatricians and family physicians. Pediatrics, 110(3), 509-516. Retrieved from http://go.galegroup.com.proxy1.lib.uwo.ca/ps/i.do?p=AONE&u=lond95336&id=...|A91560726&v=2.1&it=r&sid=summon&authCount=1
- Bosch, K., & Bergen, M. B. (2006). The influence of supportive and nonsupportive persons in helping rural women in abusive partner relationships become free from abuse. Journal of Family Violence, 21, 311-320. doi: 10.1007/s10896-006-9027-1
- Bosch, K., & Schumm, W. R. (2004). Accessibility to resources: Helping rural women in abusive partner relationships become free from abuse. Journal of Sex & Marital Therapy, 30, 357-370. doi: 10.1080/00926230490465118
- Bottos, S. (2007). Women and violence: Theory, risk, and treatment implications. Ottawa, ON: Correctional Service of Canada.
- Bourassa, C., Lavergne, C., Damant, D., Lessard, G., & Turcotte, P. (2006). Awareness and detection of the co-occurrence of interparental violence and child abuse: Child welfare worker's perspective. Children and Youth Services Review, 28(11), 1312-1328. doi: 10.1016/j.childyouth.2006.02.002
- Boyce, J. (2016). Victimization of Aboriginal people in Canada, 2014. Juristat. Statistics Canada. Catalogue No. 85-002-X. Retrieved from http://www.statcan.gc.ca/pub/85-002-x/2016001/article/14631-eng.pdf
- Brabeck, K. M., & Guzmán. (2009). Exploring Mexican-origin intimate partner abuse survivors' help-seeking within their sociocultural contexts. Violence Victims, 24(6), 817. doi: 10.1891/0886-6708.24.6.817
- Bragg, H. L. (2003). Child protection in families experiencing domestic violence.. U.S. Department of Health and Human Services and Office on Child Abuse and Neglect. Retrieved from https://www.childwelfare.gov/pubPDFs/domesticviolence.pdf
- Brandon, J., & Hafez, S. (2008). Crimes of the community: Honour-based violence in the UK. Retrieved from http://www.civitas.org.uk/pdf/CrimesOfTheCommunity.pdf
- Brassard, R., Montminy, L., Bergeron, A. S., & Sosa-Sanchez, I. A. (2015). Application of intersectional analysis to data on domestic violence against Aboriginal women living in remote communities in the province of Quebec. Aboriginal Policy Studies, 4, 3-23. doi: 10.5663/aps.v4i1.20894
- Brown, J., & Languedoc, S. (2004). Components of an Aboriginal-based family violence intervention program. Families in Society, 85(4), 477-483. doi: 10.1606/1044-3894.1835
- Brown, T., & Tyson, D. (2012). An abominable crime: Filicide in the context of parental separation and divorce. Children Australia, 37(4), 151. doi:10.1017/cha.2012.36
- Browne, A., Williams, K. R., & Dutton, D. G. (1999). Homicide between intimate partners. In M. D. Smith & M. A. Zahn (Eds.). Homicide: A sourcebook for social research (pp. 149-164). Thousand Oaks, CA: Sage.
- Brownridge, D. A. (2003). Male partner violence against Aboriginal women in Canada: An empirical analysis. Journal of Interpersonal Violence, 18(1), 65-83. doi:10.1177/088626050223854
- Brownridge, D. A. (2008). Understanding the elevated risk of partner violence against Aboriginal women: A comparison of two nationally representative surveys of Canada. Journal of Family Violence, 23(5), 353-367. doi:10.1007/s10896-008-9160-0
- Brownridge, D. A., & Halli, S. S. (2002). Double jeopardy?: Violence against immigrant women in Canada. Violence and Victims, 17, 455-471. doi: 10.1891/vivi.17.4.455.33680
- Bryant, C., & Willis, M. (2008). Risk factors in Indigenous violent victimisation (pp. 1-86). Canberra, ACT: Australian Institute of Criminology.
- Buchanan, K. (2009). Risk assessment and spousal violence: Predictive validity and cultural applicability (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (No. NR55139). University of Regina, Regina, SK.
- Bugeja, L., Dawson, M., McIntyre, S. J., & Walsh, C. (2015). Domestic/family violence death reviews: An international comparison. Trauma, Violence, & Abuse, 16, 179-187. doi: 10.1177/1524838013517561
- Bui, H. N. (2003). Help-seeking behavior among abused immigrant women: A Case of Vietnamese American women. Violence Against Women, 9(2), 207-239. doi: 10.1177/1077801202239006
- Bui, H., & Morash, M. (2008). Immigration, masculinity, and intimate partner violence from the standpoint of domestic violence service providers and Vietnamese-origin women. Feminist Criminology, 3(3), 191-215. doi: 10.1177/1557085108321500
- Bunge, V. P. (2002). National trends in intimate partner homicides, 1974-2000. Juristat, Statistics Canada, Catalogue no. 85-002-XIE. Retrieved from http://www5.statcan.gc.ca/olc-cel/olc.action?ObjId=85-002-X20020058413&ObjType=47&lang=en.
- Burczycka, M. & Conroy, S. (2017). Family violence in Canada: A statistical profile, 2015. Juristat, Statistics Canada, Catalogue no. 85-002-X. Retrieved from https://www150.statcan.gc.ca/n1/en/pub/85-002-x/2017001/article/14698-eng.pdf?st=touiRPQm.
- Burke, J. G., O’Campo, P., & Peak, G. L. (2006). Neighbourhood influences and intimate partner violence: Does geographic setting matter? Journal of Urban Health: Bulletin of the New York Academy of Medicine, 83, 182-194. doi: 10.1007/s11524-006-9031-z
- Burkhardt, K. J. (2004). Crime, cultural reintegration and community healing: Narratives of an Inuit community (Doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. UMI No. NQ92542
- Burnette, C. E., & Cannon, C. (2014). “It will always continue unless we can change something”: Consequences of intimate partner violence for Indigenous women, children, and families. European Journal of Psychotraumatology, 5, 1-8. doi: 10.3402/ejpt.v5.24585
- Burnman, E., Smailes, S. L., & Chantier, K. (2004). ”Culture” as a barrier to service provision and delivery: Domestic violence services for minoritized women. Critical Social Policy, 24(3), 332-357. doi:10.1177/0261018304044363
- Button, D. M., & Payne, B. K. (2009). Training child protective services workers about domestic violence: Needs, strategies, and barriers. Children and Youth Services Review, 31(3), 364-369. doi: 10.1016/j.childyouth.2008.08.011
- Cairns, K., & Hoffart, I. (2009). Keeping women alive – Assessing the danger. Alberta Council of Women’s Shelters. 1-96. Retrieved from https://www.acws.ca/sites/default/files/documents/DangerAssessment-FullR...
- Campbell Collaboration. (2017). What is a systematic review? Writing a Campbell Systematic Review. Retrieved from https://www.campbellcollaboration.org/research-resources/writing-a-campb...
- Campbell, J. C. (1992). ‘If I can’t have you, no one can’: Power and control in homicide of female partners. In J. Radford, &D. E. H. Russel (Eds.). Femicide: The politics of woman killing (pp. 99-113). New York, NY: Twayne.
- Campbell, J. C. (2001). Safety planning based on lethality assessment for partners of batterers in intervention programs. Journal of Aggression, Maltreatment & Trauma, 5, 129-143. doi:10.1300/J146v05n02_08
- Campbell, J. C., Koziol-McLain, J., Webster, D., Block, C. R., Campbell, D. Curry, M. A., & Manganello, J. (2004). Research results from a national study of intimate partner homicide: The Danger Assessment Instrument. Violence Against Women and Family Violence: Developments in Research, Practice, and Policy, 125-135. Retrieved from https://www.ncjrs.gov/pdffiles1/nij/199701.pdf?bcsi_scan_15D00938B-02C633E=0&bcsi_scan_filename=199701.pdf#page=126
- Campbell, J. C., Webster, D. W., & Glass, N. (2009). The Danger Assessment: Validation of a lethality risk assessment instrument for intimate partner femicide. Journal of Interpersonal Violence, 24, 653-674. doi:10.1177/0886260508317180
- Campbell, J. C., Webster, D., Koziol-McLain, J., Block, C., Campbell, D., Curry, M. A., . . . & Sharps, P. (2003). Risk factors for femicide in abusive relationships: Results from a multisite case control study. American Journal of Public Health, 93(7), 1089-1097. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1447915/pdf/0931089.pdf
- Campbell, J. C., Webster, D., Koziol-McLain, J., Block, C., Campbell, D., Curry, M. A., . . . & Sharps, P. (2003). Risk factors for femicide in abusive relationships: Results from a multisite case control study. American Journal of Public Health, 93(7), 1089-1097. Retrieved from http://ajph.aphapublications.org/doi/pdf/10.2105/AJPH.93.7.1089
- Campbell, K. M. (2007). “What was it they lost?”: The impact of resource development on family violence in a northern Aboriginal community. Journal of Ethnicity in Criminal Justice, 5, 57-80. doi: 10.1300/J222v05n01_04
- Campbell, K. M. (2007). What was it they lost?: The impact of resource development on family violence in a northern Aboriginal community. Journal of Ethnicity in Criminal Justice, 5(1), 57. doi:10.1300/J222v05n01_04
- Campbell, M., Hilton, N. Z., Kropp, P. R., Dawson, M., & Jaffe, P. (2016). Domestic violence risk assessment: Informing safety planning & risk management. (domestic homicide brief 2). London, ON: Canadian Domestic Homicide Prevention Initiative. Retrieved from http://cdhpi.ca/domestic-violence-risk-assessment-informing-safety-planning-risk-management-brief
- Campo, M. & Tayton, S. (2015). Domestic and family violence in regional, rural and remote communities: An overview of key issues. Retrieved from https://aifs.gov.au/cfca/sites/default/files/publication-documents/cfca-...
- ,Department of Justice Canada. (2013, November). Making the links in family violence cases: Collaboration among the family, child protection and criminal justice systems: Annexes to the report of the Federal Provincial – Territorial (FPT) ad hoc working group on family violence. fJ2-385/2013E). Ottawa, ON. Retrieved from http://www.justice.gc.ca/eng/rp-pr/cj-jp/fv-vf/mlfvc-elcvf/vol2/mlfvc2-e...
- Department of Justice Canada. (2010, June). Preliminary Examination of So-calle"" Honour Killings" in Canada. (J4-23/2013E). Ottawa, ON.Retrieved from http://www.justice.gc.ca/eng/rp-pr/cj-jp/fv-vf/hk-ch/hk_eng.pdf
- Health Council of Canada. (2012). Empathy, dignity and respect. Creating Cultural safety for Aboriginal people in urban health care. (H174-39/2012E-PDF). Toronto, ON. Retrieved from http://publications.gc.ca/collections/collection_2013/ccs-hcc/H174-39-20...
- Public Health Agency of Canada. (2009). On-reserve First Nations communities: Canadian pandemic influenza preparedness: Planning guidance for the health sector. Ottawa, ON. Retrieved from Government of Canada website: https://www.canada.ca/content/dam/phac-aspc/migration/phac-aspc/cpip-pcl....
- Canadian Council for Refugees (2012). Proposed “conditional permanent tesidence” for sponsored spouses: Comments on the notice published by Citizenship and Immigration Canada. Canada Gazette 146(10). Retrieved from http://www.gazette.gc.ca/rp-pr/p1/2012/2012-03-10/pdf/g1-14610.pdf
- Canales, D., Macaulay, A., McDougall, A., Wei, R., & Campbell, M.A. (2013). A brief synopsis of risk assessment screening tools for frontline professionals responding to intimate partner violence. University of New Brunswick, Saint John, NB: Centre for Criminal Justice Studies. Retrieved from https://www.unb.ca/saintjohn/ccjs/_resources/pdf/ipvrisktoolsynopsis2013.pdf
- Celaya-Alston, R. C. (2010). Hombres en Accion (Men in Action): A Community Defined Domestic Violence Intervention with Mexican Immigrant Men (Doctoral dissertation). Retrieved from ProQuest Dissertations and Theses database (UMI No. 3450001)
- Centre de recherché interdisciplinaire sur la violence familiale et la violence faite aux femmes. (2011, January). Violence in the lives of Aboriginal girls and young women in Canada through an intersectional lens (Fact sheet, no. 6). Retrieved fromhttps://www.criviff.qc.ca/sites/criviff.qc.ca/files/publications/pub_170...
- Centres for Disease Control and Prevention (CDC). (2017). Intimate partner violence: Risk and protective factors. Retrieved from CDC website:https://www.cdc.gov/violenceprevention/intimatepartnerviolence/riskprote...
- Cesario, S. K., Nava, A., Bianchi, A., McFarlane, J., & Maddoux, J. (2014). Functioning outcomes for abused immigrant women and their children 4 months after initiating intervention. Rev Panam Salud Publica, 35(1), 8-14. Retrieved from https://www.scielosp.org/pdf/rpsp/2014.v35n1/08-14/en
- Chan, K. L. (2012). Predicting the risk of intimate partner violence: The Chinese Risk Assessment Tool for Victims. Journal of Family Violence, 27(2), 157-164. doi: 10.1007/s10896-012-9418-4
- Chanmugam, A. P. L., & Hall, K. (2012). Safety planning with children and adolescents in domestic violence shelters. Violence and Victims, 27(6), 831-848. doi: 10.1891/0886-6708.27.6.831
- Chase, R., Mignone, J., & Diffey, L. (2010). Life story board: A tool in the prevention of domestic violence. Pimatisiwin, 8(2), 145-154. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3268773/
- Chin, Y. M. (2012). Male backlash, bargaining, or exposure reduction?: Women’s working status and physical spousal violence in India. Journal of Population Economics, 25, 175-200. doi: 10.1007/s00148-011-0382-8
- Chokshi, R. (2007). South Asian immigrant women & abuse: Identifying intersecting issues and culturally appropriate solutions (Master’s thesis). Retrieved from ProQuest Dissertations Publishing, 2007 (AAIEC53559).
- Choo, E. K., Newgard, C. D., Lowe, R. A., Hall, M. K., & McConnell, K. J. (2011). Rural-urban disparities in emergency department intimate partner violence resources. Western Journal of Emergency Medicine, 12, 178-183. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3099604/pdf/wjem12_2p0178.pdf
- Chung, G. H. (2006). Grounded theory model of Korean American (KA) physicians' intimate partner violence screening and intervention practices within the KA immigrant community in the Los Angeles area (Doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (3242825)
- Classen, C. C., Palesh, O. G., & Aggarwal, R. (2005). Sexual victimization: A review of the empirical literature. Trauma, Violence, & Abuse, 6, 103–129. doi: 10.1177/1524838005275087
- Clifford, M., Porteous, T., & Varcoe, C. (2007). Critical elements of an effective response to violence against women (briefing document). Retrieved from Ending Violence Association of BC website: http://endingviolence.org/files/uploads/BN_5_MARG_WOMEN.pdf
- Coalition Against Family Violence. (2013, September). NWT family violence report card (First edition). Retrieved from Status of Women Council of the NWT website: https://www.statusofwomen.nt.ca/coalition-against-family-violence/
- Community Coordination for Women’s Safety and Ending Violence Association of British Columbia. (2013). Safety planning across culture & community: A guide for front line violence against women responders. Retrieved from Ending Violence Association of BC website: http://endingviolence.org/files/uploads/ure_and_Community_Manual_-_EVA_B...
- Community Coordination for Women’s Safety, Ending Violence Association of BC. (2007). Immigrant, refugee and non-status women and violence against women in relationships. Retrieved from Ending Violence Association of BC website http://endingviolence.org/files/uploads/Imm_Ref_Women_Violence.pdf
- Community Legal Information Association of Prince Edward Island. (2010). Health & safety plan for Aboriginal families. Retrieved from http://www.cliapei.ca/sitefiles/File/publications/FAM10.pdf
- Congress of Aboriginal Peoples. (2015). Miykiwan user guide: Toolkit for Aboriginal families living off-reserve. Retrieved from http://abo-peoples.org/wp-content/uploads/2015/03/CAP-FVPT-User-Guide.pdf
- Cooley, B., & Frazer, C. (2006). Children and domestic violence: A system of safety in clinical practice. Australian Social Work, 59(4), 462-473. doi:10.1080/03124070600986028
- Cooper, A., & Smith, E. L. (2012). Homicide trends in the United States, 1980-2008. Bureau of Justice Statistics. Retrieved from https://www.bjs.gov/index.cfm?ty=pbdetail&iid=2221
- Copenace, S. (2000). A group work approach with Aboriginal children exposed to parental violence (Master’s thesis). Retrieved from ProQuest Dissertations & Theses Global. (UMI No. MQ56116)
- Coulter, M. L., & Mercado-Crespo, M. C. (2015). Co-occurrence of intimate partner violence and child maltreatment: Service providers’ perceptions. Journal of Family Violence, 30(2), 255-262. doi:10.1007/s10896-014-9667-5
- Coy, M., Kelly, L., Foord, J., & Bowstead, J. (2011). Roads to nowhere? Mapping violence against women services. Violence Against Women, 17, 404-425. doi: 10.1177/1077801211398637
- Cramer, E. P., & Plummer, S. B. (2009). People of color with disabilities: Intersectionality as a framework for analyzing intimate partner violence in social, historical, and political contexts. Journal of Aggression, Maltreatment & Trauma, 18, 162-181. doi: 10.1080/10926770802675635
- Crandall, M., Senturia, K., Sullivan, M., & Shiu-Thornton, S. (2005). "No way out": Russian-speaking women's experiences with domestic violence. Journal of Interpersonal Violence, 20(8), 941-958. doi:10.1177/0886260505277679
- Crenshaw, K. (1989). Demarginalizing the intersection of race and sex: A black feminist critique of antidiscrimination doctrine, feminist theory, and antiracist politics. University of Chicago Legal Forum, 14, 538-554. Retrieved from https://philpapers.org/archive/CREDTI.pdf?ncid=txtlnkusaolp00000603
- Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43, 1241-1299. doi: 10.2307/1229039
- Cripps, K. (2007). Indigenous family violence: From emergency measures to committed long term action. Australian Indigenous Law Rev, 11, 7-18. Retrieved from http://heinonline.org/HOL/Page?handle=hein.journals/austindlr11&div=14&g...
- Cripps, K., & McGlade, H. (2008). Indigenous family violence and sexual abuse: Considering pathways forward. Journal of Family Studies, 14(2-3), 240-253. doi: 10.5172/jfs.327.14.2-3.240
- Cross, P. (2013). Violence against women: Health and justice for Canadian Muslim women. Retrieved from Centre for Research & Education on Violence Against Women & Children website: http://www.learningtoendabuse.ca/sites/default/files/VAW_health_Justice.pdf
- Cross, T. P., Mathews, B., Tonmyr, L., Scott, D., & Ouimet, C. (2012). Child welfare policy and practice on children's exposure to domestic violence. Child Abuse & Neglect, 36(3), 210-216. doi:10.1016/j.chiabu.2011.11.004
- Cunradi, C. B. Neighborhoods, alcohol outlets and intimate partner violence: Addressing research gaps in explanatory mechanisms. (2010). International Journal of eEnvironmental Research and Public Health, 7 (3), 799-813. doi: 10.3390/ijerph7030799
- Daniels, J. W., & Murphy, C. M. (1997). Stages and processes of change in batterers' treatment. Cognitive and Behavioral Practice, 4(1), 123-145. Retrieved from http://search.proquest.com/docview/619431854?accountid=15115
- Daoud, N., Smylie, J., Urquia, M., Allan, B. & O'Campo, P. (2013). The contribution of socio-economic position to the excesses of violence and intimate partner violence among Aboriginal versus non-Aboriginal women in Canada. Canadian Public Health Association, 104(4), 278-283. Retrieved from https://www.lib.uwo.ca/cgi-bin/ezpauthn.cgi?url=http://search.proquest.c...
- Davis, K. (2008). Intersectionality as buzzword: A sociology of science perspective on what makes a feminist theory successful. Feminist Theory, 9, 67-85. doi: 10.1177/1464700108086364
- Davis, K., & Taylor, B. (2002). Voices from the margins, part 1: Narrative accounts of Indigenous family violence, & part 2: Narrative accounts of the support needs of Indigenous families experiencing violence. Contemporary Nurse, 14(1), 66-85. doi:10.5172/conu.14.1.66
- Davis, K., Taylor, B., & Furniss, D. (2001). Narrative accounts of tracking the rural domestic violence survivors’ journey: A feminist approach. Health Care for Women International, 22, 333-347. doi: 10.1080/07399330119209
- Dawson, M. (2010). Considerations for the development of a pan-Canadian map of family violence resources. Retrieved from http://www.violenceresearch.ca/system/files/files/DAWSON%20%282010%29%20...
- Dawson, M. (2015). Canadian trends in filicide by gender of the accused, 1961–2011. Child Abuse & Neglect, 47, 162-174. doi: 10.1016/j.chiabu.2015.07.010
- Dawson, M. (Ed). (2017). Domestic homicides and death reviews: An international perspective. London, UK: Palgrave Macmillan
- Dawson, M., Bunge, V., & Balde, T. (2009). National trends in intimate partner homicides: Explaining the decline, Canada, 1976-2001. Violence Against Women, 15(3): 276-306. doi: 10.1177/1077801208330433
- Dawson, M., Hubbert, M. J., & Poon, J. (2010, June). Documenting resources for victims & survivors of violence in Canada: A workshop discussion paper. Retrieved from http://violenceresearch.ca/sites/default/files/DAWSON,%20POON%20%26%20HU...(2010)%20DOCUMENTING%20RESOURCES%20FOR%20VICTIMS%20%26%20SURVIVORS%20OF%20VIOLENCE%20IN%20CANADA.pdf
- Day, A., Jones, R., Nakata, M., & McDermott, D. (2012). Indigenous family violence: An attempt to understand the problems and inform appropriate and effective responses to criminal justice system intervention. Psychiatry, Psychology and Law, 19(1), 104-117. doi: 10.1080/13218719.2010.543754
- Denham, A. C., Frasier, P. Y., Hooten, E. G., Belton, L., Newton, W., Gonzalez, P., …Campbell, M. K. (2007). Intimate partner violence among Latinas in Eastern North Carolina. Violence Against Women, 13, 123-140. doi: 10.1177/1077801206296983
- DeVoe, E. R., & Smith, E. L. (2003). Don't take my kids: Barriers to service delivery for battered mothers and their young children. Journal of Emotional Abuse, 3(3-4), 277-294. doi: 10.1300/J135v03n03_06
- Dickson-Gilmore, J. (2014). Whither restorativeness? Restorative justice and the challenge of intimate violence in Aboriginal communities. Canadian Journal of Criminology and Criminal Justice, 56, 417-446. doi:10.3138/cjccj.2014.S02
- Dill, B. T., & Zambrana, R. E. (2009). Critical thinking about inequality: An emerging lens. In B. T. Dill. & R. E. Zambrana (Eds.), Emerging intersections: Race, class, and gender in theory, policy, and practice (pp. 1-21). Piscataway, NJ: Rutgers University Press.
- Doherty, D., & Hornosty, J. (2004). Abuse in a rural and farm context. In M. Stirling, C. Cameron, N. Nason Clark, & B. Miedema (Eds.), Understanding Abuse: Partnering for change (55-82). Toronto, ON: University of Toronto Press. doi: 10.3138/9781442682870q
- Doherty D. (2006). Domestic homicide in New Brunswick: An overview of some contributing factors. Atlantis, 30, 4-14. Retrieved from http://journals.msvu.ca/index.php/atlantis/article/view/818/805
- Doherty D., & Hornosty, J. (2008, May). Exploring the links: Firearms, family violence and animal abuse in rural communities: . Final research report to the Canadian Firearms Centre, Royal Canadian Mounted Police, and Public Safety Canada. Retrieved from http://www.legal-info-legale.nb.ca/en/uploads/file/pdfs/Family_Violence_...
- Donnelly, S. L. (2015). Two sides of the same coin---a qualitative meta-study of factors influencing immigrant women's experiences of intimate partner violence (Doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global database.(UMI No. 3704895),.
- Douglas, H., & Walsh, T. (2010). Mothers, domestic violence, and child protection. Violence Against Women, 16, 489-508. doi: 10.1177/1077801210365887
- Douglas, K. S., & Kropp, P. R. (2002). A prevention-based paradigm for violence risk assessment: Clinical and research applications. Criminal Justice and Behavior, 29, 617-658. doi: 10.1177/009385402236735
- Dragiewicz, M., & DeKeseredy, W. (2008, November). Study on the experiences of abused women in the family courts in eight regions in Ontario: Research report. Retrieved from http://ywcacanada.ca/data/research_docs/00000030.pdf
- Dreaddy, K. & Provincial Association Against Family Violence. (2002). Moving toward safety: Responding to family violence in Aboriginal and northern communities of Labrador.Retrieved from ffairb
- Du Mont, J., & Forte, T. (2012). An exploratory study on the consequences and contextual factors of intimate partner violence among immigrant and Canadian-born women. BMJ Open, 2, 1-9. doi: 10.1136/bmjopen-2012-001728
- Du Mont, J., Hyman, I., O'Brien, K., White, M. E., Odette, F., & Tyyska, V. (2012). Factors associated with intimate partner violence by a former partner by immigration status and length of residence in Canada. Annals of Epidemiology, 22(11), 772-777. doi:10.1016/j.annepidem.2012.09.001
- Dudgeon, A., & Evanson, T. A. (2014). Intimate partner violence in rural U.S. areas: What every nurse should know. American Journal of Nursing, 114, 26-35. doi: 10.1097/01.NAJ.0000446771.02202.35
- Dugan, L., Nagin, D.S., & Rosenfeld, R. (1999). Explaining the decline in intimate partner homicide: The effects of changing domesticity, women’s status, and domestic violence resources. Homicide Studies, 3 (3), 187-214. doi: 10.1177/1088767999003003001
- Dugan, L. & Nagin, D.S., & Rosenfeld, R. (2001). Exposure reduction or backlash? The effect of domestic violence resources on intimate partner homicide, Final Report. Retrieved from https://www.ncjrs.gov/pdffiles1/nij/grants/186194.pdf
- Dugan, L., Nagin, D.S., & Rosenfeld, R. (2003). Exposure reduction or retaliation? The effects of domestic violence resources on intimate-partner homicide. Law & Society Review, 37, 169-198. doi: 10.1111/1540-5893.3701005
- Dutton, D. G., & Kropp, P. R. (2000). A review of domestic violence risk instruments. Trauma, Violence, & Abuse, 1, 171-181. doi:10.1177/1524838000001002004
- Dutton, M. A., Orloff, L. E., & Aguilar Hass, G. (2000). Characteristics of help-seeking behaviors, resources and service needs of battered immigrant Latinas: Legal and policy implications. Georgetown Journal on Poverty Law and Policy, 7(2), 245-305. Retrieved from https://www.researchgate.net/publication/288318092_Characteristics_of_he...
- Earner, I. (2010). Double risk: Immigrant mothers, domestic violence and public child welfare services in New York City. Evaluation and Program Planning, 33, 288-293. doi: 10.1016/j.eavlprogplan.2009.05.016
- Eastman, B. J., & Bunch, S. G. (2007). Providing services to survivors of domestic violence: A comparison of rural and urban service provider perceptions. Journal of Interpersonal Violence, 22, 465-473. doi: 10.1177/0886260506296989
- Eastman, B. J., Bunch, S. G., Williams, A. H., & Carawan, L. W. (2007). Exploring the perceptions of domestic violence service providers in rural localities. Violence Against Women, 13, 700-716. doi: 10.1177/1077801207302047
- Echauri, J. A., Femántiez-Montalvo, J., Martínez, M., & Azkarate, J. M. (2013). Effectiveness of a treatment programme for immigrants who committed gender-based violence against their partners. Psicothema, 25(1), 49-54. doi: 10.7334/psicothema2012.75
- Echeburua, E., Fernandez-Montalvo, J., de Corral, P., & Lopez-Goni, J. J. (2009). Assessing risk markers in intimate partner femicide and severe violence: A new assessment snstrument. Journal of Interpersonal Violence, 24(6), 925-939. doi: 10.1177/0886260508319370
- Edelstein, A. A. (2013). Culture transition, acculturation and intimate partner homicide. SpringerPlus, 2(1), 338. doi:10.1186/2193-1801-2-338
- Eden, K.B., Perrin, N.A., Hanson, G.C., Messing, J.T., Bloom, T.L., Campbell, J.C.,…Glass, N.E. (2015). Use of online safety decision aid by abused women: eEffect on decisional conflict in randomized controlled trail. American Journal of Preventive Medicine, 48(4), 372-83. doi: 10.1016/j.amepre.2014.09.027
- Edleson, J. L. (2004). Should childhood exposure to adult domestic violence be defined as child maltreatment under the law. In Jaffe, P.G., Baker, L.L. & Cunningham, A.J (Eds.) Protecting children from domestic violence: Strategies for community intervention, 8-29. New York, NY: Guilford Press.
- Edleson, J. L., Ellerton, A. L., Seagren, E. A., Kirchberg, S. L., Schmidt, S. O., & Ambrose, A. T. (2007). Assessing child exposure to adult domestic violence. Children and Youth Services Review, 29(7), 961-971. doi:10.1016/j.childyouth.2006.12.009.
- Edleson, J. L., Gassman-Pines, J., & Hill, M. B. (2006). Defining child exposure to domestic violence as neglect: Minnesota's difficult experience. Social Work, 51(2), 167-174. Retrieved from http://go.galegroup.com.proxy1.lib.uwo.ca/ps/i.do?p=AONE&u=lond95336&id=GALE|A149316878&v=2.1&it=r&sid=summon&authCount=1
- Edleson, J.L., Mbilinyi, L.F., Beeman, S.K., & Hagemeister, A.K. (2003). How children are involved in adult domestic violence: Results from a four-city telephone survey. Journal of Interpersonal Violence, 18(1), 18-32. doi: 10.1177/0886260502238538.
- Edwards, K. M. (2014). Intimate partner violence and the rural-urban-suburban divide: Myth or reality? A critical review of the literature. Trauma, Violence, & Abuse, 16, 359-373. doi:10.1177/1524838014557289
- Edwards, K. M., Mattingly, M. J., Dixon, K. J., & Banyard, V. L. (2014). Community matters: Intimate partner violence among rural young adults. American Journal of Community Psychology, 53, 198-207. doi: 10.1007/s10464-014-9633-7
- Eke, A. W., Hilton, N. Z., Harris, G. T., Rice, M. E., & Houghton, R. E. (2011). Intimate partner homicide: Risk assessment and prospects for prediction. Journal of Family Violence, 26, 211-216. doi: 10.1007/s10896-010-9356-y
- Ely, G. E. (2004). Domestic violence and immigrant communities in the United States: A review of women's unique needs and recommendations for social work practice and research. Stress, Trauma and Crisis: An International Journal, 7(4), 223-241. doi: 10.1080/15434610490888027
- End Domestic Abuse Wisconsin. (2014). 2014 Wisconsin domestic violence homicide report. Retrieved from http://www.endabusewi.org/sites/default/files/resources/2014_wisconsin_d...
- Ending Violence Association of BC. (2013). Safety planning across culture & community: A guide for front line violence against women responders. Retrieved from http://endingviolence.org/files/uploads/ure_and_Community_Manual_-_EVA_B...
- Ending Violence Association of BC, et al. (2011). Immigrant women's project: Safety of immigrant, refugee, and non-status women. Retrieved from Ending Violence Association of BC website http://endingviolence.org/wp-content/uploads/2014/03/IWP_Resource_Guide_...
- Ending Violence Association of BC. (2015). Interagency case assessment team best practices: Working together to reduce the risk of domestic violence. Retrieved from Ending Violence Association of BC website http://endingviolence.org/publications/icat-best-practices-guide/
- Erez, E. (2000). Immigration, culture conflict and domestic violence/woman battering. Crime Prevention & Community Safety, 2(1), 27-36. doi: 10.1057/palgrave.cpcs.8140043
- Erez, E., & Hartley, C. C. (2003). Battered immigrant women and the legal system: A therapeutic jurisprudence perspective. Western Criminology Review, 4(2), 155-169. Retrieved from http://westerncriminology.org/documents/WCR/v04n2/article_pdfs/erezhartl...
- Erez, E., Adelman, M., & Gregory, C. (2009). Intersections of immigration and domestic violence: Voices of battered immigrant women. Feminist Criminology, 4, 32-56. doi: 10.1177/1557085108325413
- Ernst, A. A., Weiss, S. J., Enright-Smith, S., & Hansen, J. P. (2008). Positive outcomes from an immediate and ongoing intervention for child witnesses of intimate partner violence. The American Journal of Emergency Medicine, 26(4), 389-394. doi: 10.1016/j.ajem.2007.06.018
- Etherington, N., & Baker, L. (2016). From “buzzword” to best practice: Applying intersectionality to children exposed to intimate partner violence. Trauma, Violence, & Abuse. Advance online publication. doi: 10.1177/1524838016631128
- Evanson, T. A. (2006). Intimate partner violence and rural public health nursing practice: Challenges and opportunities. Online Journal of Rural Nursing and Health Care, 6, 7-20. Retrieved from http://rnojournal.binghamton.edu/index.php/RNO/article/viewFile/162/138
- Fairbairn J., Jaffe P., Dawson M. (2017) Challenges in Defining Domestic Homicide: Considerations for Research and Practice. In Dawson M. (Eds.) Domestic Homicides and Death Reviews: An International Perspective (pp.201-228). London, UK: Palgrave Macmillan
- Fallon, B., Van Wert, M., Trocmé, N., MacLaurin, B., Sinha, V., Lefebvre, R., Allan, K., . . . Goel, S. (2015). Ontario incidence study of reported child abuse and neglect-2013 (OIS-2013). Toronto, ON: Child Welfare Research Portal.
- Family Violence Death Review Committee (2014). Fourth Annual Report: January 2013 to December 2013. Wellington, NZ: Family Violence Death Review Committee.
- Fantuzzo, J. W., & Fusco, R. A. (2007). Children’s direct exposure to types of domestic violence crime: A population-based investigation. Journal of Family Violence, 22(7), 543-552. doi: 10.1007/s10896-007-9105-z
- Fantuzzo, J., DePaola, L.M., Lambert, L., Martino, T., Anderson, G., & Sutton, S. (1991). Effects of interparental violence on the psychological adjustment and competencies of young children. Journal of Consulting and Clinical Psychology, 59, 258-265. doi: 10.1037//0022-006X.59.2.258
- Faver, C. A., & Strand, E. B. (2003). To leave or to stay? Battered women's concern for vulnerable pets. Journal of Interpersonal Violence, 18, 1367-1377. doi: 10.1177/0886260503258028
- Federal-Provincial-Territorial Ministers Responsible for Justice and Public Safety. (2016). FPT justice framework to address violence against Indigenous women and girls. Retrieved from https://www2.gov.bc.ca/assets/gov/law-crime-and-justice/about-bc-justice...
- Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., . . . Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245-258. doi: 10.1016/S0749-3797(98)00017-8
- Fernbrant, C., Essén, B., Östergren, P.-O., & Cantor-Graae, E. (2011). Perceived threat of violence and exposure to physical violence against foreign-born women: A Swedish population-based study. Women's Health Issues, 21(3), 206-213. doi: 10.1016/j.whi.2010.12.001
- Ferrante, A., Morgan, F., Indermaur, D., & Harding, R. (1996). Measuring the extent of Domestic Violence. Sydney, AU: Hawkins Press.
- Fine, S. (2015, May 29). Chief Justice says Canada attempted ‘cultural genocide’ on aboriginals. Globe and Mail. Retrieved from https://www.theglobeandmail.com/news/national/chief-justice-says-canada-...
- Finfgeld-Connett, D. (2014). Intimate partner abuse among older women: Qualitative systematic review. Clinical Nursing Research, 23(6), 664-683. doi: 10.1177/1054773813500301
- Fitzsimons, N. M., Hagemeister, A. K., & Braun, E. J. (2011). Interpersonal violence against people with disabilities: Understanding the problem from a rural context. Journal of Social Work & Disability Rehabilitation, 10, 166-188. doi: 10.1080/1536710X.2011.596437
- Fleury, R. E., Sullivan, C. M., & Bybee, D. I. (2000). When ending the relationship does not end the violence: Women’s experience of violence by former partners. Violence Against Women, 6, 1363-1383. doi: 10.1177/10778010022183695
- Fong, J. S. (2000). Silent no more: How women experienced wife abuse in the local Chinese community (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertation & Theses Global. (UMI No. NQ59134)
- Fotheringham, S., Dunbar, J., & Hensley, D. (2013). Speaking for themselves: Hope for children caught in high conflict custody and access disputes involving domestic violence. Journal of Family Violence, 28(4), 311-324. doi:10.1007/s10896-013-9511-3
- Four Worlds Centre for Development Learning, Bopp, M., Bopp, J., & Lane, P. (2003). Aboriginal domestic violence in Canada. The Aboriginal Healing Foundation. Retrieved from http://www.ahf.ca/downloads/domestic-violence.pdf
- Frye, V., Galea, S., Tracy, M., Buccialrelli, A. Putnam, S, & Wilt, S. (2008). The role of neighborhood environment and risk of intimate partner violence in a large urban area. American Journal of Public Health, 98(8), 1473-1479. doi: 10:2105/ajph.2007.112813
- Fuchsel, C. L. M., Murphy, S. B., & Dufresne, R. (2012). Domestic violence, culture, and relationship dynamics among immigrant Mexican women. Affilia Journal of Women and Social Work. 27(3) 263-274. doi: 10.1177/0886109912452403
- Gadomski, A. M., Tripp, M., Wolff, D. A., Lewis, C., & Jenkins, P. (2001). Impact of a rural domestic violence prevention campaign. Journal of Rural Health, 17,266-277. / doi/10.1111/j.1748-0361.2001.tb00964.x/epdf
- Gallup-Black, A. (2004, June 30). Rural and urban trends in family and intimate partner homicide: 1980-1999 (Document No. 208344). U.S. Department of Justice. Retrieved from https://www.ncjrs.gov/pdffiles1/nij/grants/208344.pdf
- Ganley, A. L., & Schechter, S. (1996). Domestic violence: a national curriculum for child protective services. San Francisco, CA: Family Violence Prevention Fund.
- Gartner, R., Dawson, M., & Crawford, M. (1999). Woman killing: Intimate femicide in Ontario, 1974-1994. Resources for Feminist Research, 26, 151-173. Retrieved from http://www.violenceresearch.ca/
- Gill, A. (2008). 'Crimes of honour’ and violence against women in the UK. International Journal of Comparative and Applied Criminal Justice, 32(2), 243-263. doi: 10.1080/01924036.2008.9678788
- Gill, C. (2012). Domestic homicide in New Brunswick 1999-2008. Retrieved from New Brunswick Department of Public Safety website: http://www2.gnb.ca/content/dam/gnb/Departments/ps-sp/pdf/Publications/19...
- Glass, N., Eden, K. B., Bloom, T., & Perrin, N. (2010). Computerized aid improves safety decision process for survivors of intimate partner violence. Journal of Interpersonal Violence, 25(11), 1947-1964. doi:10.1177/0886260509354508
- Goetting, A. (1995). Homicide in families and other special populations. New York, NY: Springer.
- Gonzalez, A., MacMillan, H., Tanaka, M., Jack, S. M., & Tonmyr, L. (2014). Subtypes of exposure to intimate partner violence within a Canadian child welfare sample: Associated risks and child maladjustment. Child Abuse & Neglect, 38(12), 1934-1944. doi: 10.1016/j.chiabu.2014.10.007
- Goodkind, J. R., Sullivan, C. M., & Bybee, D. I. (2004). A contextual analysis of battered women’s safety planning. Violence Against Women, 10, 514-533. doi: 10.1177/1077801204264368
- Gordon, S., Hallahan, K., & Henry, D. (2002). Putting the picture together: Inquiry into response by government agencies to complaints of family violence and child abuse in Aboriginal communities. Australian Indigenous L. Rep., 7(4), 49-72. Retrieved from http://www.strongfamilies.wa.gov.au/UserDir/Documents/Public/Putting%20t...
- Grama, J. l. (2000). Women forgotten: Difficulties faced by rural victims of domestic violence. American Journal of Family Law, 14, 173-188.
- Grau, D., & Smith, T. (2011). Community guide to end violence against Aboriginal women. Retrieved from Ontario Native Women’s Association website: http://www.onwa.ca/upload/documents/onwa_2011community-guide.pdf
- Greenard-Smith, C. (2003). Women escaping abuse in northern British Columbia: Attributes and resources that make the most difference (Unpublished master’s thesis). Retrieved from ProQuest Dissertations & Theses Global. (UMI No. MQ80701)
- Grossman, S. F., Hinkley, S., Kawalski, A., & Margrave, C. (2005). Rural versus urban victims of violence: The interplay of race and region. Journal of Family Violence, 20, 71-81. doi: 10.1007/s10896-005-3170-y
- Grove, W. M., & Meehl, P. E. (1996). Comparative efficiency of informal (subjective, impressionistic) and formal (mechanical, algorithmic) prediction procedures: The clinical-statistical controversy. Psychology, Public Policy, and Law, 2, 293-323. doi: 10.1037//1076-8971.2.2.293
- Guimei, M., Fikry, F. E., & Esheiba, O. M. (2012). Patterns of violence against women in three communities in Alexandria, Egypt. MCN: American Journal of Maternal/Child Nursing, 37, 331-338. doi: 10.1097/NMC.0b013e31825c99d8.
- Gunnarsson, D. K. (2012). A multi-disciplinary intervention package for the management of stalking behaviors in child custody cases (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (UMI No. 3569392)
- Guruge S., & Khanlou N. (2004). Intersectionalities of influence: Researching the health of immigrant and refugee women. Canadian Journal of Nursing Research, 36, 33-47. Retrieved from http://cjnr.archive.mcgill.ca/article/view/1898/1892
- Guruge, S., & Humphreys, J. (2009). Barriers affecting access to and use of formal social supports among abused immigrant women. CJNR: Canadian Journal of Nursing Research, 41(3), 64-84. Retrieved from http://www.ingentaconnect.com/content/mcgill/cjnr/2009/00000041/00000003...
- Gustafsson, H. C. (2013). Intimate partner violence in rural, low-income communities: Prevalence and links with child competence (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertation & Theses Global. (UMI No. 3562902)
- Gustafsson, H. C., Cox, M. J., & the Family Life Project Key Investigators. (2016). Intimate partner violence in rural low-income families: Correlates and change in prevalence over the first 5 years of a child's life. Journal of Family Violence, 31, 49-60. doi:10.1007/s10896-015-9760-4
- Gustafsson, H. C., Cox, M. J., & the Family Life Project Key Investigators. (2016). Intimate partner violence in rural low-income families: Correlates and change in prevalence over the first 5 years of a child’s life. Journal of Family Violence, 31, 49-60. doi: 10.1007/s10896-015-9760-4
- Hamby, S., Finkelhor, D., Turner, H., & Ormrod, R. (2010). The overlap of witnessing partner violence with child maltreatment and other victimizations in a nationally representative survey of youth. Child Abuse & Neglect, 34(10), 734-741. doi: 10.1016/j.chiabu.2010.03.001
- Hamilton, L. H. A., Jaffe, P. G., & Campbell, M. (2013). Assessing children's risk for homicide in the context of domestic violence. Journal of Family Violence, 28(2), 179-189. doi:10.1007/s10896-012-9473-x
- Hampton, M., Woods, M., McKenzie, H., Taylor, W., & George, D. (2010). Legal system use patterns in Saskatchewan rural, urban, and northern survivors of intimate partner violence [PowerPoint slides]. Retrieved from http://www.unb.ca/fredericton/arts/centres/mmfc/_resources/pdfs/10hampto...
- Hancock, T. (2006). Addressing wife abuse in Mexican immigrant couples: Challenges for family social workers. Journal of Family Social Work, 10(3), 31-50. doi: 10.1300/J039v10n03_03
- Hancock, T. U., & Ames, N. (2008). Toward a model for engaging Latino lay ministers in domestic violence intervention. Families in Society: The Journal of Contemporary Social Services, 89(4), 623-630. doi: 10.1606/1044-3894.3824
- Hancock, T. U., & Siu, K. (2009). A culturally sensitive intervention with domestically violent Latino immigrant men. Journal of Family Violence, 24(2), 123-132. doi: 10.1007/s10896-008-9217-0
- Hansen, B. & Wells, L. (2015). Consulting the community on advancing an lgbtq framework on the prevention of domestic violence. Shift: The Project to End Domestic Violence. Calgary, AB: The University of Calgary,
- Hardesty, J. L., & Chung, G. H. (2006). Intimate partner violence, parental divorce, and child custody: Directions for intervention and future research. Family Relations, 55(2), 200-210. doi:10.1111/j.1741-3729.2006.00370.x
- Hart, L. G., Larson, E. H., & Lishner, D. M. (2005). Rural definitions for health policy and research. American Journal of Public Health, 95, 1149-1155. doi: 10.2105/AJPH.2004.042432
- Hass, G. A., Dutton, M. A., & Orloff, L. E. (2000). Lifetime prevalence of violence against Latina immigrants: Legal and policy implications. International Review of Victimology, 7, 93-113. doi: 10.1177/026975800000700306
- Hassan, G., Thombs, B., Rousseau, C., Kirmayer, L. J., Feightner, J., Ueffing, E., & Pottie, K. (2011). Appendix 13: Intimate partner violence: Evidence review for newly arriving immigrants. Canadian Medical Association Journal. 7(1-13). doi: 10.1503/cmaj.090313
- Hassija, C., & Gray, M. J. (2011). The effectiveness and feasibility of videoconferencing technology to provide evidence-based treatment to rural domestic violence and sexual assault populations. Telemedicine Journal and E-Health, 17, 309-315. doi: 10.1089/tmj.2010.0147
- Hazen, A. L., Connelly, C. D., Kelleher, K., Landsverk, J., & Barth, R. (2004). Intimate partner violence among female caregivers of children reported for child maltreatment. Child Abuse & Neglect, 28(3), 301-319. doi: 10.1016/j.chiabu.2003.09.016
- Hazen, A., & Soriano, F. I. (2005). Experience of intimate partner violence among U.S. born, immigrant and migrant Latinas. (Report no. 211509). Retrieved from National Criminal Justice Reference Service website: http://www.ncjrs.gov/pdffiles1/nij/grants/211509.pdf
- Healy, J., & Bell, M. (2005). Assessing the risks to children from domestic violence. Barnado’s Northern Ireland policy and practice brief (7). Retrieved from Barnado’s Northern Ireland: Belfast website: http://www.barnardos.org.uk/pp_no_7_assessing_the_risks_to_children_from...
- Heckert, D. A., & Gondolf, E. W. (2004). Battered women’s perceptions of risk versus risk factors and instruments in predicting repeat re-assault. Journal of Interpersonal Violence, 19, 778-800. doi:10.1177/0886260504265619
- Hegarty, K., Forsdike-Young, K., Tarzia, L., Schweitzer, R., & Vlais, R. (2016). Identifying and responding to men who use violence in their intimate relationships. The Royal Australian College of General Practitioners, 45, 176-181. Retrieved from https://www.racgp.org.au/download/Documents/AFP/2016/April/AFP-Focus-Heg...
- Heise, L. L. (1998). Violence against women: An integrated, ecological framework. Violence Against Women, 4, 262-290. doi: 10.1177/1077801298004003002
- Helms, B. L. (2015). Honour and shame in the Canadian Muslim community: Developing culturally sensitive counselling nterventions. Canadian Journal of Counselling and Psychotherapy, 49(2), 163-184. Retrieved from http://cjc-rcc.ucalgary.ca/cjc/
- Helmus, L,. & Bourgon, G. (2011). Taking stock of 15 years of research on the Spousal Assault Risk Assessment Guide (SARA): A critical review. International Journal of Forensic Mental Health, 10, 64-75. doi: 10.1080/14999013.2010.551709
- Higgins, J. P. T., Green, S. (Eds.). (2011). Cochrane handbook for systematic reviews of interventions. Version 5.1.0. The Cochrane Collaboration, 2011. Retrieved from http://handbook.cochrane.org/
- Hilton, N. Z., & Harris, G. T. (2005). Predicting wife assault: A critical review and implications for policy and practice. Trauma, Violence, & Abuse, 6, 3-23. doi:10.1177/1524838004272463
- Hilton, N. Z., & Harris, G. T. (2009). How non-recidivism affects predictive accuracy: Evidence from a cross-validation of the Ontario Domestic Assault Risk Assessment (ODARA). Journal of Interpersonal Violence, 24, 326-337. doi:10.1177/0886260508316478
- Hilton, N. Z., Harris, G. T., Rice, M. E., Houghton, R. E., & Eke, A. W. (2008). An in-depth actuarial assessment for wife assault recidivism: The Domestic Violence Risk Appraisal Guide. Law and Human Behavior, 32, 150-163. doi:10.1007/s10979-007-9088-6
- Hilton, N. Z., Harris, G. T., Rice, M. E., Lang, C., Cormier, C. A., & Lines, K. J. (2004). A brief actuarial assessment for the prediction of wife assault recidivism: The Ontario Domestic Assault Risk Assessment. Psychological Assessment, 16, 267-275. doi:10.1037/1040-3590.16.3.267
- Holder, M. R. (2015). Exploring the potential relationship between historical trauma and intimate partner violence among Indigenous women (Doctoral dissertation). Abstract retrieved from ProQuest Dissertation & Theses (UMI No. 3724924)
- Holt, S., Buckley, H., & Whelan, S. (2008). The impact of exposure to domestic violence on children and young people: A review of the literature. Child Abuse & Neglect, 32(8), 797-810. doi: 10.1016/j.chiabu.2008.02.004
- Horn, P., & Groves, B. M. (2006). Children exposed to domestic violence: Making trauma-informed custody and visitation decisions. Juvenile and Family Court Journal, 57(1), 51-60. doi:10.1111/j.1755-6988.2006.tb00114.x.
- Hornosty, J., & Doherty, D. (2002). Responding to wife abuse in farm and rural communities: Searching for solutions that work. SIPP Public Policy Paper No.10. Saskatchewan Institute of Public Policy Paper Series. 1-38. Retrieved from http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.582.1977&rep=re...
- Horton, E., Murray, C. E., Garr, B., Notestine, L., Flasch, P., & Johnson, C. H. (2014). Provider perceptions of safety planning with children impacted by intimate partner violence. Children and Youth Services Review, 42, 67-73. doi: 10.1016/j.childyouth.2014.03.016
- Huerta, D. I. (2014). Family related attitudes and beliefs influencing risk and support seeking among female victims of domestic and sexual violence in El Paso, Texas (Doctoral dissertation). Retrieved from ProQuest Dissertation and Theses Global. (UMI No. 1583921)
- Hughes, J., & Chau, S. (2013). Making complex decisions: Child protection workers' practices and interventions with families experiencing intimate partner violence. Children and Youth Services Review, 35(4), 611-617. doi:10.1016/j.childyouth.2013.01.003
- Hughes, J., Chau, S., & Poff, D. C. (2011). “They're not my favourite people”: What mothers who have experienced intimate partner violence say about involvement in the child protection system. Children and Youth Services Review, 33(7), 1084-1089. doi: 10.1016/j.childyouth.2011.01.015
- Hulbert, S. N. (2008). Children exposed to violence in the child protection system: Practice-based assessment of the system process can lead to practical strategies for improvement. Journal of Emotional Abuse, 8(1-2), 217-234. doi: 10.1080/10926790801986171
- Humphreys, C., & Bradbury Jones, C. (2015). Domestic abuse and safeguarding children: Focus, response and intervention. Child Abuse Review, 24(4), 231-234. doi:10.1002/car.2410
- Humphreys, C., & Harrison, C. (2003). Focusing on safety – domestic violence and the role of child contact centres. Child & Family Law Quarterly. 15(3), 237-253. Retrieved from https://www.researchgate.net/publication/255727763
- Humphreys, C., Mullender, A., Lowe, P., Hague, G., Abrahams, H., & Hester, M. (2001). Domestic violence and child abuse: Developing sensitive policies and guidance. Child Abuse Review, 10(3), 183-197. doi: 10.1002/car.686
- Humphreys, J., Sharps, P., & Campbell, J. (2005). What we know and what we still need to learn. Journal of Interpersonal Violence, 20, 182-187. doi: 10.1177/0886260504268766
- Hyman, I., & Forte, T. (2006). The association between length of stay in Canada and intimate partner violence among immigrant women. American Journal of Public Health, 96(4), 654. doi:10.2105/AJPH.2004.046409
- Hyman, I., Forte, T., Mont, J. D., Romans, S., & Cohen, M. (2006). Help-seeking rates for intimate partner violence (IPV) among Canadian immigrant women. Health Care Women International 27(8), 682-694. doi:10.1080/07399330600817618
- Hyman, I., Mason, R., Guruge, S., Berman, H., Kanagaratnam, P., & Manuel, L. (2011). Perceptions of factors contributing to intimate partner violence among Sri Lankan Tamil immigrant women in Canada. Health Care Women International, 32(9), 779-794. doi:10.1080/07399332.2011.569220
- Jackson, D. (2012). A meta-study of filicide: Reconceptualizing child deaths by parents (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertation & Theses Global. (UMI No. 3487404)
- Jaffe, P. G., & Juodis, M. (2006). Children as victims and witnesses of domestic homicide: Lessons learned from domestic violence death review committees. Juvenile and Family Court Journal, 57, 13-28. doi: 10.1111/j.1755-6988.2006.tb00125.x
- Jaffe, P. G., Campbell, M., Olszowy, L., & Hamilton, L. H. A. (2014). Paternal filicide in the context of domestic violence: Challenges in risk assessment and risk management for community and justice professionals. Child Abuse Review, 23(2), 142-153. doi: 10.1002/car.2315
- Jaffe, P. G., Crooks, C. V., & Bala, N. (2009). A framework for addressing allegations of domestic violence in child custody disputes. Journal of Child Custody: Research, Issues, and Practices, 6(3-4), 169-188. doi: 10.1080/15379410903084517
- Jaffe, P., Dawson, M., & Campbell, M. (2011). Lessons learned from domestic violence tragedies: Emerging research, policies & practices to prevent domestic homicides. Retrieved from http://www.learningtoendabuse.ca/sites/default/files/Think-Tank%20on%20D...
- Jaffe, P.G., Campbell, M., Hamilton, L.H.A, & Juodis, M. (2012). Children in danger of domestic homicide. Child Abuse & Neglect, 36(1), 71-74. doi: 10.1016/j.chiabu.2011.06.008
- Jamieson, S., & Wendt, S. (2008). Exploring men’s perpetrator programs in small rural communities. Rural Society, 18, 39-50. doi: 10.5172/rsj.351.18.1.39
- Janovicek, N., Doherty, D., Blaney, E., David-Shediac, A., Miller, K., & Nicholson, M. (2003, November). Caring partnerships: An evaluation of a community development model for family violence prevention. Retrieved from http://www.unb.ca/fredericton/arts/centres/mmfc/_resources/pdfs/prismfin...
- Jenney, A. C. (2011). Doing the right thing: Negotiating risk and safety in child protection work with domestic violence cases (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (UMI No. NR77949)
- Jin, X., & Kent. (2010). The effects of change in Sspousal power on intimate partner violence among Chinese immigrants. Journal of Interpersonal Violence, 25(4), 610. doi:10.1177/0886260509334283
- Johnson, H., & Dawson, M. (2011). Violence against women in Canada: Research and policy perspectives. Don Mills, ON: Oxford University Press.
- Johnson, M. E. (2010). Balancing liberty, dignity, and safety: The impact of domestic violence lethality screening. Cardozo Law Review, 32, 519-580. Retrieved from http://heinonline.org/HOL/Page?handle=hein.journals/cdozo32&div=16&g_sent=1&casa_token=&collection=journals
- Johnston, J. R. (2006). A child-centered approach to high-conflict and domestic-violence families: Differential assessment and interventions. Journal of Family Studies, 12(1), 15-35. Retrieved from https://www.lib.uwo.ca/cgi-bin/ezpauthn.cgi?url=http://search.proquest.c...
- Jones, R., Masters, M., Griffiths, A., & Moulday, N. (2002). Culturally relevant assessment of Indigenous offenders: A literature review. Australian Psychologist, 37(3), 187-197. doi: 10.1080/00050060210001706866
- Juodis, M., Starzomski, A., Porter, S., & Woodworth, M. (2014). What can be done about high-risk perpetrators of domestic violence? Journal of Family Violence, 29, 381-390. doi:10.1007/s10896-014-9597-2
- Kan, M. L., & Feinberg, M. E. (2014). Can a family-focused, transition-to-parenthood program prevent parent and partner aggression among couples with young children? Violence and Victims, 29(6), 967-980. doi:10.1891/0886-6708.VV-D-12-00162
- Kasdorff, D., & Erb, B. (2010, January). Serving victims of violence in rural communities: Challenges and best practices. Victim Witness Assistance Program, East Region. Retrieved from http://library.queensu.ca/files/Rural%20Issues%20in%20Eastern%20Ontario%...
- Keller, E. M., & Brennan, P. K. (2007). Cultural considerations and challenges to service delivery for Sudanese victims of domestic violence: Insights from service providers and actors in the criminal justice system. International Review of Victimology, 14(1), 115-141. doi: 10.1177/026975800701400107
- Kelly, U. (2006). “What will happen if I tell you?” Battered Latina women's experiences of health care. CJNR (Canadian Journal of Nursing Research), 38(4), 78-95. Retrieved from http://www.ingentaconnect.com/content/mcgill/cjnr/2006/00000038/00000004...
- Kelly, U. A. (2011). Theories of intimate partner violence: From blaming the victim to acting against injustice: Intersectionality as an analytic framework. Advances in Nursing Science, 34(3), E29–E51. doi: 10.1097/ANS.0b013e3182272388
- Kennedy, A. C., Bybee, D., Kulkarni, S. J., & Archer, G. (2013). Sexual victimization and family violence among urban African American adolescent women: Do violence cluster profiles predict partner violence victimization and sex trade exposure? Violence Against Women, 18, 1319-1338. doi: 10.1177/1077801212470544
- Kim, C., & Sung, H.-G. (2016). Characteristics and risk factors of Chinese immigrant intimate partner violence victims in New York City and the role of supportive networks. The Family Journal, 24(1), 60. doi: 10.1177/1066480715615632
- Kim, J. Y., & Sung, K.-t. (2000). Conjugal violence in Korean American families: A residue of the cultural tradition. Journal of Family Violence, 15(4), 331-345. doi: 10.1023/A:1007502212754
- Kirkwood, D. (2013). 'Just say goodbye': Parents who kill their children in the context of separation. Retrieved from Domestic Violence Resource Centre Victoria: http://www.dvrcv.org.au/sites/default/files/%E2%80%98Just%20Say%20Goodbye%E2%80%99%20(January%202013%20online%20edition).pdf
- Kitzman, K. M., Gaylord, N. K., Holt, A. R., & Kenny, E. D. (2003). Child witness to domestic violence: A meta-analytic review. Journal of Consulting and Clinical Psychology, 71(2), 339–352. doi: 10.1037/0022-006X.71.2.339
- Kiyoshk, R. (2003). Integrating spirituality and domestic violence treatment: Treatment of Aboriginal men. Journal of Aggression, Maltreatment & Trauma, 7(1-2), 237-256. doi: 10.1300/J146v07n01_10
- Klevens, J. (2007). An overview of intimate partner violence among Latinos. Violence Against Women, 13(2), 111-122. doi:10.1177/1077801206296979
- Kohl, P. L., Barth, R. P., Hazen, A. L., & Landsverk, J. A. (2005). Child welfare as a gateway to domestic violence services. Children and Youth Services Review, 27(11), 1203-1221. doi: 10.1016/j.childyouth.2005.04.005
- Korteweg, A. C. (2012). Understanding honour killing and honour-related violence in the immigration context: Implications for the legal profession and beyond. Canadian Criminal Law Review, 16(2), 135-160. Retrieved from https://korteweg.files.wordpress.com/2010/12/korteweg_cclr-understanding...
- Koziol-McLain, J., Vandal, A. C., Nada-Raja, S., Wilson, D., Glass, N. E., Eden, K. B.,Case, J. (2015). A web-based intervention for abused women: The New Zealand isafe randomised controlled trial protocol. BMC Public Health, 15, 1-8. doi: 10.1186/s12889-015-1395-0
- Kress, V. E., Adamson, N. A., Paylo, M. J., DeMarco, C., & Bradley, N. (2012). The use of safety plans with children and adolescents living in violent families. The Family Journal, 20(3), 249-255. doi:10.1177/1066480712448833
- Krishnan, S. P., Hilbert, J. C., & Pase, M. (2001). An examination of intimate partner violence in rural communities: Results from a hospital emergency department study from southwest United States. Family and Community Health, 24, 1-14. Retrieved from: http://ovidsp.tx.ovid.com/
- Kropp, P. R., & Hart, S. D. (2015). User manual for version 3 of the Spousal Assault Risk Assessment Guide (SARA-V3). Vancouver, BC: Protect International, Inc.
- Kropp, P. R. (2004). Some questions regarding spousal assault risk assessment. Violence Against Women, 10, 676-697. doi: 10.1177/1077801204265019
- Kropp, P. R. (2008). Intimate partner violence risk assessment and management. Violence and Victims, 23, 202-220. doi: 10.1891/0886-6708.23.2.202
- Kropp, P. R., & Hart, S. D. (2000). The Spousal Assault Risk Assessment (SARA) Guide: Reliability and validity in adult male offenders. Law and Human Behavior, 24, 101-118. doi:10.1023/A:1005430904495
- Kropp, P. R., Hart, S. D., Webster, C. W., & Eaves, D. (1994). Manual for the Spousal Assault Risk Assessment Guide. Vancouver, BC: British Columbia Institute on Family Violence.
- Kropp, P.R. (2008). Risk assessment and management of spousal assaulters and stalkers. In A. C. Baldry, & F. W. Winkel (Eds.), Intimate partner violence prevention and intervention: The risk assessment and management approach. Hauppauge, NY: Nova Science Publishers.
- Kulwicki, A., Aswad, B., Carmona, T., & Ballout, S. (2010). Barriers in the utilization of domestic violence services among Arab immigrant women: Perceptions of professionals, service providers & community leaders. Journal of Family Violence, 25(8), 727-735. doi: 10.1007/s10896-010-9330-8
- Kyriakakis, S. (2014). Mexican immigrant women reaching out: The role of informal networks in the process of seeking help for intimate partner violence. Violence Against Women, 20(9), 1097-1116. doi: 10.1177/1077801214549640
- Lake Jr, I. B., Odom, C. H., & Starsoneck, L., (2003, Febuary). Child well-being and domestic violence task force final report. Retrieved from State Library of North Carolina website: http://digital.ncdcr.gov/cdm/ref/collection/p249901coll22/id/286989
- Lamontagne, M. (2011). Violence against Aboriginal women: Scan and report. Toronto, ON: Canadian Women’s Foundation.
- Lanier, C., & Maume, M. O. (2009). Intimate partner violence and social isolation across the rural/urban divide. Violence Against Women, 15, 1311-1330. doi: 10.1177/1077801209346711
- Lant, J. M. (2014). Intimate partner victimization in Canada: A test of risk factors, self-control, routine activities, social disorganization, and collective efficacy (Master’s thesis). Retrieved from ProQuest Dissertations & Theses Global. (UMI No. 1565940).
- Lapierre, S., & Côté, I. (2011). “I made her realise that I could be there for her, that I could support her”: Child protection practices with women in domestic violence cases. Child Care in Practice, 17(4), 311-325. doi: 10.1080/13575279.2011.598142
- Latta, R. E., & Goodman, L. A. (2005). Considering the interplay of cultural context and service provision in intimate partner violence: The case of Haitian immigrant women. Violence Against Women, 11(11), 1441-1464. doi: 10.1177/1077801205280273
- Laughon, K., Sutherland, M. A., & Parker, B. J. (2011). A brief intervention for prevention of sexually transmitted infection among battered women. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 40, 702-708. doi: 10.1111/j.15526909.2011.01305.x
- Lavergne, C., Damant, D., Clement, M.-E., Bourassa, C., Lessard, G., & Turcotte, P. (2011). Key decisions in child protection services in cases of domestic violence: Maintaining services and out-of-home placement. Child and Family Social Work, 16(3), 353-363. doi: 10.1111/j.1365-2206.2010.00750.x
- Lee, E. (2007). Domestic violence and risk factors among Korean immigrant women in the United States. Journal of Family Violence, 22(3), 141-149. doi: 10.1007/s10896-007-9063-5
- Lee, M.-Y. (2000). Understanding Chinese battered women in North America: A review of the literature and practice implications. Journal of Multicultural Social Work, 8(3-4), 215. doi:10.1300/J285v08n03_03
- Lee, Y. S., & Hadeed, L. (2009). Intimate partner violence among Asian immigrant communities: Health/mental health consequences, help-seeking behaviors, and service utilization. Trauma, Violence, & Abuse, 10, 143-170. doi: 10.1177/1524838009334130
- Lee, Y.-S., & Hadeed, L. (2009). Intimate partner violence among Asian immigrant communities Health/mental health consequences, help-seeking behaviors, and service utilization. Trauma, Violence, & Abuse, 10(2), 143-170. doi: 10.1177/1524838009334130
- Lessard, G., Flynn, C., Turcotte, P., Damant, D., Vézina, J-F., Godin, M-F., . . . Rondeau-Cantin, S. (2010). Child custody issues and co-occurrence of intimate partner violence and child maltreatment: Controversies and points of agreement amongst practitioners. Child & Family Social Work, 15(4), 492-500. doi:10.1111/j.1365-2206.2010.00705.x
- Lester-Smith, D. (2013). Healing Aboriginal family violence through Aboriginal storytelling. International Journal of Indigenous Peoples, 9(4), 309-321. doi: 10.1177/117718011300900403
- Lester-Smith, D. M. (2012). “Hope for change—change can happen”: Healing the wounds family violence with Indigenous traditional wholistic practices (Unpublished doctoral dissertation). UBC Theses & Dissertations. (H10-02458)
- Leth, P. M. (2009). Intimate partner homicide. Forensic Science, Medicine, and Pathology, 5(3), 199-203. doi: 10.1007/s12024-009-9097-5
- Lewis, M., West, B., Bautista, L., Greenberg, A. M., & Done-Perez, I. (2005). Perceptions of service providers and community members on intimate partner violence within a Latino community. Health Education & Behavior, 32(1), 69-83. doi: /10.1177/1090198104269510
- Liao, M. S. (2006). Domestic violence among Asian Indian immigrant women: Risk factors, acculturation, and intervention. Women & Therapy, 29, 23-39. doi: 10.1300/J015v29n01_02
- Light, L. (2007). Empowerment of immigrant and refugee women who are victims of violence in their intimate relationships. Retrieved from http://books1.scholarsportal.info.proxy1.lib.uwo.ca/viewdoc.html?id=/ebo...
- Light, L., et al. (2008). Keeping women safe: Eight critical components of an effective justice response to domestic violence. Retrieved from http://endingviolence.org/files/uploads/KeepingWomenSafe0416.pdf
- Lindhorst, T., Macy, R. J., & Nurius, P. (2005). Contextualized assessment with battered women: Strategic safety planning to cope with multiple harms. Journal of Social Work Education, 41, 331-352. doi: 10.5175/JSWE.2005.200200261
- Logan, T. K., Walker, R., & Leukefeld, C. G. (2001). Rural, urban influenced, and urban differences among domestic violence arrestees. Journal of Interpersonal Violence, 16, 266-283. doi: 10.1177/088626001016003006
- Logan, T. K., Walker, R., Cole, J., Ratliff, S., & Leukefeld, C. (2003). Qualitative differences among rural and urban intimate violence victimization experiences and consequences: A pilot study. Journal of Family Violence, 18, 83-92. Retrieved from https://link.springer.com/article/10.1023/A:1022837114205
- Loveland, J.E., & Raghavan, C. (2014). Near-lethal violence in a sample of high-risk men in same-sex relationships. Psychology of Sexual Orientation and Gender Diversity, 1(1), 51-62. doi: 10.1037/sgd0000012
- Lykke, N. (2010). Feminist studies: A guide to intersectional theory, methodology and writing. New York, NY: Routledge.
- Lyons-Ruth, K., Zeanah, C.H., Benoit, D., Madigan, S. & Mills-Koonce, W.R. (2014). Disorder and risk for disorder during infancy and toddlerhood. In Mash, E. J., & Barkley, R. (Eds.). Child Psychopathology: 3rd edition (pp. 673-736). New York, NY: Guilford Press.
- MacMillan, H. L., Wathen, C. N., & Varcoe, C. M. (2013). Intimate partner violence in the family: Considerations for children's safety. Child Abuse & Neglect, 37(12), 1186-1191. doi:10.1016/j.chiabu.2013.05.005
- MacMillan, H., Wathen, N., Jamieson, E., Boyle, M., Harry, S., Ford-Bilboe, M.,…McNutt, L. (2009). Screening for intimate partner violence in health care settings. A randomized trial. JAMA, 302(5), 493-501. doi:10.1001/jama.2009.1089
- Marchetti, E. (2010). The role of Australian Indigenous elders in court when sentencing partner violence offenders. Retrieved from https://papers.ssrn.com/sol3/papers.cfm?abstract_id=1623243
- Marchetti, E. (2015). An Australian Indigenous-focused justice response to intimate partner violence: Offenders’ perceptions of the sentencing process. British Journal of Criminology, 55(1), 86-106. doi: 10.1093/bjc/azu089
- Marchetti, E., & Anthony, T. (2016). Sentencing Indigenous offenders in Canada, Australia, and New Zealand. University of Technology Sydney Law Research Series. Retrieved from http://classic.austlii.edu.au/au/journals/UTSLRS/2016/27.html
- Marrs Fuchsel, C. L. (2014). "Yes, I feel stronger with more confidence and strength:" Examining the experiences of immigrant Latina women (ILW) participating in the Sí, Yo Puedo curriculum. Journal of Ethnographic & Qualitative Research, 9(2), 161-182.
- Marrs Fuchsel, C. L., & Hysjulien, B. (2013). Exploring a domestic violence intervention curriculum for immigrant Mexican women in a group setting: A pilot study. Social Work with Groups: A Journal of Community and Clinical Practice, 36(4), 304-320. doi: 10.1080/01609513.2013.767130
- Mason, R., Hyman, I., Berman, H., Guruge, S., Kanagaratnam, P., & Manuel, L. (2008). “Violence is an international language”: Tamil women's perceptions of intimate partner violence. Violence Against Women, 14(12), 1397-1412. doi: 10.1177/1077801208325096
- Maume, M. O., Lanier, C. L., Hossfeld, L. H., & Wehmann, K. (2014). Social isolation and weapon use in intimate partner violence incidents in rural areas. International Journal of Rural Criminology, 2, 244-267. doi: 10.18061/1811/61592
- McCall-Hosenfeld, J. S., Weisman, C. S., Perry, A. N., Hillemeier, M. M., & Chuang, C. H. (2014). "I just keep my antennae out”: How rural primary care physicians respond to intimate partner violence. Journal of Interpersonal Violence, 29, 2670-2694. doi: 10.1177/0886260513517299
- Mehrotra, G. (2010). Toward a continuum of intersectionality theorizing for feminist social work scholarship. Affilia: Journal of Women and Social Work, 25, 417-430. doi: 10.1177/0886109910384190
- Menjívar, C., & Salcido, O. (2002). Immigrant women and domestic violence: Common experiences in different countries. Gender & Society, 16(6), 898-920. doi: 10.1177/089124302237894
- Messing, J. T., & Thaller, J. (2013). The average predictive validity of intimate partner violence risk assessment instruments. Journal of Interpersonal Violence, 28, 1537-1558. doi:10.1177/0886260512468250
- Messing, J. T., Amanor-Boadu, Y., Cavanaugh, C. E., Glass, N. E., & Campbell, J. C. (2013). Culturally competent intimate partner violence risk assessment: Adapting the Danger Assessment for immigrant women. Social Work Research, 37(3), 263-275. doi: 10.1093/swr/svt019
- Messing, J. T., Campbell, J., Webster, D. W., Brown, S., Patchell, B., & Wilson, J. S. (2015). The Oklahoma lethality assessment study: A quasi-experimental evaluation of the Lethality Assessment Program. Social Service Review, 89, 499-530. Retrieved from https://www.journals.uchicago.edu/doi/pdfplus/10.1086/683194
- Messing, J. T., Glass, N. E., & Campbell, J. C. (2013). Danger assessment for immigrant women (DA-I). Retrieved from http://www.vawnet.org/summary.php?doc_id=4417&find_type=web_sum_GC
- Messing, J. T., O’Sullivan, C. S., Cavanaugh, C. E., Webster, D. W., & Campbell, J. (2016). Are abused women’s protective actions associated with reduced threats, stalking, and violence perpetrated by their male intimate partners? Violence Against Women. Advance online publication. doi:10.77/801216640381
- Midlarsky, E., Venkataramani-Kothari, A., & Plante, M. (2006). Domestic violence in the Chinese and South Asian immigrant communities. Annals of the New York Academy ofSciences, 1087, 279-300. doi:10.1196/annals.1385.003
- Miladinovic, Z. & Mulligan, L. (2015). Homicide in Canada, 2014.Juristat. Statistics Canada, Catalogue no. 85-002-X. Retrieved from http://www.statcan.gc.ca/pub/85-002-x/2015001/article/14244-eng.pdf
- Miller, L. E., Howell, K. H., Hunter, E. C., & Graham-Bermann, S. A. (2012). Enhancing safety-planning through evidence-based interventions with preschoolers exposed to intimate partner violence. Child Care in Practice, 18(1), 67-82. doi:10.1080/13575279.2011.621885
- Mills, L., Friend, C., Conroy, K., Fleck-Henderson, A., Krug, S., . . . Trudeau, J. (2000). Child protection and domestic violence: Training, practice, and policy issues. Children and Youth Services Review, 22(5), 315-332. doi:10.1016/S0190-7409(00)00083-9
- Min, P. G. (2001). Changes in Korean immigrants' gender role and social status, and their marital conflicts. Sociological Forum, 16(2), 301-320. doi:10.1023/a:1011056802719
- Min, P. G. (2001). Changes in Korean immigrants' gender role and social status, and their marital conflicts. Sociological Forum, 16(2), 301-320. doi:10.1023/a:1011056802719
- Moffitt, P., Fikowski, H., Mauricio, M., & Mackenzie, A. (2013). Intimate partner violence in the Canadian territorial north: Perspectives from a literature review and a media watch. International Journal of Circumpolar Health, 72, 215-221. doi: 10.3402/ijch.v72i0.21209
- Molina, O., Lawrence, S. A., Azhar-Miller, A., & Rivera, M. (2009). Divorcing abused Latina immigrant women's experiences with domestic violence support groups. Journal of Divorce & Remarriage, 50(7), 459-471. doi: 10.1080/10502550902970561
- Morash, M., Bui, H. N., & Santiago, A. M. (2000). Cultural-specific gender ideology and wife abuse in Mexican-descent families. International Review of Victimology, 7(1-3), 67-91. doi:10.1177/026975800000700305
- Morash, M., Bui, H. N., & Santiago, A. M. (2000). Cultural-Specific Gender Ideology and Wife Abuse in Mexican-Descent Families. International Review of Victimology, 7(1-3), 67-91. doi:10.1177/026975800000700305
- MOSAIC. (2015). Preventing and reducing violence against women and girls in the name of "honour". MOSAIC. Retrieved from https://www.mosaicbc.org/resources/in-the-name-of-honour/
- Moynihan, B., Gaboury, M. T., & Onken, K. J. (2008). Undocumented and unprotected immigrant women and children in harm's way. Journal of Forensic Nursing, 4(3), 123-129. doi:10.1111/j.1939-3938.2008.00020.x
- Murphy, R. A. (2010). Multi-system responses in the context of child maltreatment and intimate partner violence. Child Abuse & Neglect, 34(8), 555-557. doi:10.1016/j.chiabu.2007.07.013
- Murray, C. E., & Graves, K. N. (2012). Responding to family violence: A comprehensive, research-based guide for therapists. New York, NY: Routledge.
- Murray, C. E., Horton, G. E., Johnson, C. H., Notestine, L., Garr, B., Pow, A. M., … Doom, E. (2015). Domestic violence service providers’ perceptions of safety planning: A focus group study. Journal of Family Violence, 30, 381-392. doi: 10.1007/s10896-015-9674-1
- Muskoday Community Health Centre. (2012). Community and family violence elimination initiative: An evidence-based approach to identify community assets and build our nation’s capacity to intervene and prevent family and community violence in Muskoday First Nation. Muskoday, SK: Muskoday First Nation.
- Natarajan, M. (2002). Domestic violence among immigrants from India: What we need to know and what we should do. International Journal of Comparative and Applied Criminal Justice, 26(3), 301-321. doi: 10.1080/01924036.2002.9678693
- Native Women’s Association of Canada([NWAC) (2011). Collaboration to end violence: National Aboriginal women’s forum. (Final report for Department of Justice, Canada) Ottawa, ON: Author.
- Native Women’s Association of Canada (NWAC). (2010). What their stories tell us: Research findings from the sisters in spirit initiative. Ottawa, ON: Author. https://nwac.ca/wp-content/uploads/2015/07/2010-What-Their-Stories-Tell-...
- Native Women’s Association of Canada (NWAC). (2015). You are not alone: A toolkit for Aboriginal women escaping domestic violence. Ottawa, ON: Author.Retrieved from https://nwac.ca/policy-areas/violence-prevention-and-safety/you-are-not-...
- Neill, K. & Hammatt, J. (2015). Beyond urban places: Responding to intimate partner violence in rural and remote areas. Journal of Forensic Nursing, 11, 93-100. doi: 10.1097/JFN.0000000000000070
- Nelson, J.R., & Lund, E.M., 2017. Bronfenbrenner’s theoretical framework adapted to women with disabilities experiencing tntimate partner violence. In A. J. Johnson, J. R. Nelson, & E. M. Lund (Eds.), Religion, Disability, and Interpersonal Violence (pp. 11-23). Cham, CH: Springer International Publishing.
- Cham, SZNew South Wales Domestic Violence Death Review Team. (2015). Annual Report 2013-2015. Sydney, AU: Author.
- Nicholls, T. L., Desmarais, S. L., Douglas, K. S., & Kropp, P. R. (2007). Violence risk assessments with perpetrators of intimate partner abuse. In J. Hamel & T. L. Nicholls (Eds.), Family interventions in domestic violence (pp. 275-302). New York, NY: Springer Publishing.
- Nicholls, T. L., Pritchard, M. M., Reeves, K. A., & Hilterman, E. (2013). Risk assessment in intimate partner violence: A systematic review of contemporary approaches. Partner Abuse, 4, 76-168. doi: 10.1891/1946-6560.4.1.76
- Nicholls, V. (2008). Aboriginal children exposed to family violence: A discussion paper. Retrieved from Native Women’s Association website: https://nwac.ca/wp-content/uploads/2015/05/2008-Children-Exposed-to-Fami...
- Nilsson, J. E., Brown, C., Russell, E. B., & Khamphakdy-Brown, S. (2008). Acculturation, partner violence, and psychological distress in refugee women from Somalia. Journal of Interpersonal Violence, 23(11), 1654-1663. dio:10.2105/ajph.2007.112813
- Nixon, K,. & Bonnycastle, C. (2012, November). Challenging the notion of failure to protect: A qualitative study exploring the protective strategies of urban and northern abused mothers . Retrieved from http://fredacentre.com/wp-content/uploads/2012/11/Nixon_5b.pdf
- Nixon, K. L., Bonnycastle, C., & Ens, S. (2015). Challenging the notion of failure to protect: Exploring the protective strategies of abused mothers living in urban and remote communities and implications for practice. Child Abuse Review, 26, 63-74. doi: 10.1002/car.2417
- Norris, A. N., Zajicek, A., & Murphy-Erby, Y. (2010). Intersectional perspective and rural poverty research: Benefits, challenges and policy implications. Journal of Poverty, 14, 55-75. doi: 10.1080/1087554090349413
- Northcott, M. (2011). Domestic violence in rural Canada. In S. McDonald (Ed.). Victims of Crime Research Digest. Ottawa: Department of Justice. 9-14.
- Novick, S., Yoshihama, M., Runner, M., & Fund, F. V. P. (2009). Intimate partner violence in immigrant and refugee communities: Challenges, promising practices, and recommendations. Retrieved from http://www.policyarchive.org/handle/10207/21315
- New South Wales Department of Health. (2011). NSW health Aboriginal family health strategy: Responding to family violence in Aboriginal communities. Retrieved from http://www.health.nsw.gov.au/aboriginal/Publications/pub-family.pdf
- Oetzel, J., & B. Duran. (2004). Intimate partner violence in American Indian and/or Alaska native communities: A social ecological framework of determinants and interventions. American Indian and Alaska native mental health research (Online) 11(3), 49-68. Retrieved from https://www.lib.uwo.ca/cgi-bin/ezpauthn.cgi?url=http://search.proquest.c...
- Office of the Chief Coroner for Ontario. (2015, October). Domestic Violence Death Review Committee 2013-14 Annual Report. Toronto, ON.: Retrieved from http://www.mcscs.jus.gov.on.ca/sites/default/files/content/mcscs/docs/ec...
- Ogunsiji, O., Wilkes, L., Jackson, D., & Peters, K. (2012). Suffering and smiling: West African immigrant women’s experience of intimate partner violence. Journal of Clinical Nursing, 21(11-12), 1659-1665. doi: 10.1111/j.1365-2702.2011.03947.x
- Olsen Harper, A. (2011). Domestic violence in Aboriginal communities: A context for resilience (Doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (No. NR79722)
- Olszowy, L., Jaffe, P.G., Campbell, M., & Hamilton, L.H.A. (2013). Effectiveness of risk assessment tools in differentiating child homicides from other domestic homicide cases. Journal of Child Custody, 10(2), 185-206. doi: 10.1080/15379418.2013.796267
- O'Malley, D. M., Kelly, P. J., & Cheng, A.-L. (2013). Family violence assessment practices of pediatric ED nurses and physicians. Journal of Emergency Nursing, 39(3), 273-279. doi:10.1016/j.jen.2012.05.028
- Ontario Council of Agencies Serving Immigrants. (2006). Prevention of domestic violence against immigrant and refugee women: Prevention through intervention training. Retrieved from http://ccrweb.ca/files/ocasi_domviolence_training_manual_nov2006_0.pdf
- Ontario Women’s Justice Network. (2016). Creating a safety plan. Retrieved from http://owjn.org/2008/12/creating-a-safety-plan/
- Orloff, L. E. (2014). Interviewing and safety planning for immigrant victims of domestic violence. Retrieved from Legal Momentum: The Women's Legal Defense and Education Fund website: http://library.niwap.org/wp-content/uploads/2015/CULT-Man-Ch2-InterviewingSafetyPlanningImmVictimsDV-09.23.14.pdf
- Owen, S., & Carrington, K. (2015). Domestic violence (DV) service provision and the architecture of rural life: An Australian case study. Journal of Rural Studies, 39, 229-238. doi: 10.1016/j.jrurstud.2014.11.004
- Pan, A., Daley, S., Rivera, L. M., Williams, K., Lingle, D., & Reznik, V. (2006). Understanding the role of culture in domestic violence: The Ahimsa Project for Safe Families. Journal of Immigrant and Minority Health, 8(1), 35-43. doi: 10.1007/s10903-006-6340-y
- Parra-Cardona, J. R., Escobar-Chew, A. R., Holtrop, K., Carpenter, G., Guzmán, R., Hernández, D., . . . Ramírez, D. G. (2013). "En el grupo tomas conciencia (In group you cecome aware)": Latino immigrants' satisfaction with a culturally informed intervention for men who batter. Violence Against Women, 19(1), 107. doi: 10.1177/1077801212475338
- Pauktuutit Inuit Women’s Association. (2005). Research report: Applying Inuit cultural approaches in the prevention of family violence and abuse. Nuluaq Project: National Inuit Strategy for Abuse Prevention. Retrieved from https://www.pauktuutit.ca/wp-content/uploads/InuitAbusePrevention_e.pdfP..., C., Wallis, A., Harland, K., Beyer, K., Dickey, P., & Saftlas, A. (2011). Rural disparity in domestic violence prevalence and access to resources. Journal of Women’s Health, 20, 1743-1749. doi: 10.1089/jwh.2011.2891
- Pendleton, G. (2003). Ensuring fairness and justice for noncitizen survivors of domestic violence. Juvenile and Family Court Journal, 54(4), 69-85. doi:10.1111/j.1755-6988.2003.tb00087.x
- Pennell, J., Rikard, R. V., & Sanders-Rice, T. (2014). Family violence: Fathers assessing and managing their risk to children and women. Children and Youth Services Review, 47(1), 36-45. doi:10.1016/j.childyouth.2013.11.004.
- Perreault, S. (2009). Criminal victimization and health: A profile of victimization among persons with activity limitations or other health problems. Canadian Centre for Justice Statistics Profile Series. Statistics Canada Catalogue no. 85F0033M – No. 21, 1-23. Retrieved from http://www.statcan.gc.ca/pub/85f0033m/85f0033m2009021-eng.pdf
- Pinzon, C. E. (2006). The expectations of protection of survivors of intimate partner abuse and their interveners (Master’s thesis). Retrieved from ProQuest Dissertations & Theses Global. (UMI No. 1435163)
- Postmus, J. L., & Merritt, D. H. (2010). When child abuse overlaps with domestic violence: The factors that influence child protection workers' beliefs. Children and Youth Services Review, 32(3), 309-317. doi:10.1016/j.childyouth.2009.09.011.
- Potts, G. G. (2011). The strategic and community safety response to domestic violence in a rural area (Unpublished doctoral dissertation). Northumbria University, Newcastle, UK. Retrieved from http://nrl.northumbria.ac.uk/7264/1/potts.gordon_phd.pdf
- Public Health Agency of Canada. (2010). Canadian incidence study of reported child abuse and neglect - 2008: Major Findings. Ottawa, ON. Author
- Public Health Agency of Canada. (2016, October). The Chief Public Health Officer’s Report on the State of Public Health in Canada 2016: A focus on family violence in Canada. Retrieved from https://www.canada.ca/content/dam/canada/public-health/migration/publica...
- Puchala, C., Paul, S., Kennedy, C., Mehl-Madrona, L. (2010). Using traditional spirituality to reduce domestic violence within Aboriginal communities. The Journal of Alternative and Complementary Medicine, 16(1), 89-96. doi: 10.1089/acm.2009.0213
- Radford, L., Blacklock, N., & Iwi, K. (2006). Domestic violence risk assessment and safety planning in child protection – Assessing perpetrators. In C. Humphreys, & N. Stanley (Eds.). Domestic violence and child protection: Directions for good practice (pp. 171-189). London: Jessica Kingsley Publishers.
- Ragusa, A. T. (2012). Rural Australian women's legal help seeking for intimate partner violence: Women intimate partner violence victim survivors’ perceptions of criminal justice support services. Journal of Interpersonal Violence, 28, 685-717. doi: 10.1177/088626051245586
- Raj, A., & Silverman, J. (2002). Violence against immigrant women: The roles of culture, context, and legal immigrant status on intimate partner violence. Violence Against Women, 8(3), 367-398. doi: 10.117/10778010222183107
- Rana, S. (2012). Addressing domestic violence in immigrant communities: Critical issues for culturally competent services. Retrieved from http://vawnet.org/print-document.php?doc_id=3157&find_type=web_desc_AR
- Reckdenwald, A. (2008). Examining changes in male and female intimate partner homicide over time, 1990-2000 (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (UMI No. 3425495)
- Reckenwald, A., & Parker, K. F. (2010). Understanding gender-specific intimate partner homicide: A theoretical and domestic service-oriented approach. Journal of Criminal Justice, 38, 951-958. doi:10.1016/j.jcrimjus.2010.06.012
- Rees, S., & Pease, B. (2007). Domestic violence in refugee families in Australia. Journal of Immigrant & Refugee Studies, 5(2), 1-19. doi: 10.1300/J500v05n02_01
- Rees, S., & Pease, B. (2007). Domestic violence in refugee families in Australia. Journal of Immigrant and Refugee Studies, 5, 1-19. doi: 10.1300/J500v05n02_01
- Registered Nurses’ Association of Ontario (RNAO). (2015, May). Coming together, moving forward: Building the next chapter of Ontario’s rural, remote & northern nursing workforce report. Toronto, ON: RNAO. Retrieved from http://rnao.ca/sites/rnao-ca/files/RR_May8.pdf
- Reina, A. S., Lohman, B. J., & Maldonado, M. M. (2014). “He said they'd deport me”: Factors influencing domestic violence help-seeking practices among Latina immigrants. Journal of Interpersonal Violence, 29(4), 593-615. doi: 10.1177/0886260513505214
- Rennison, C. M., DeKeseredy, W. S., & Dragiewicz, M. (2013). Intimate relationship status variations in violence against women: Urban, suburban, and rural differences. Violence Against Women, 19, 1312-1330. doi: 10.1177/107780121351448
- Revuelto, J. C. (2002). Factors of isolation: Rural domestic violence in an underserved Texas county (Unpublished doctoral dissertation). Texas A&M University, College Station, TX
- Richardson-Foster, H., Stanley, N., Miller, P., & Thomson, G. (2012). Police intervention in domestic violence incidents where children are present: Police and children's perspectives. Policing and Society, 22(2), 220-234. doi:10.1080/10439463.2011.636815.
- Richie, B. (2000). A Black feminist reflection on the antiviolence movement. Signs, 25, 1133-1137. doi: 10.1086/495533
- Riddell, T., Ford-Gilboe, M., & Leipert, B. (2009). Strategies used by rural women to stop, avoid, or escape from intimate partner violence. Health Care for Women International, 30, 134-159. doi: 10.1080/07399330802523774
- Riel, E., (2013). Conjoint therapy for intimate partner violence among Aboriginal couples: Service providers' perspectives on risk and safety (Master’s thesis) Retrieved from Electronic Thesis and Dissertation Repository. (1194)
- Riel, E., Languedoc, S., Brown, J., & Gerrits, J. (2014a). Couples counseling for Aboriginal clients following intimate partner violence: Service providers' perceptions of risk. International Journal of Offender Therapy and Comparative Criminology, 60(3), 286-307. doi:10.1177/0306624X14551953
- Riel, E., Languedoc, S., Brown, J., & Rodgers, J. (2014b). Safety for Aboriginal women in couples counseling where there is a history of intimate partner violence. Journal of Offender Rehabilitation, 53(6), 478-500. doi: 10.1080/10509674.2014.931749
- Riggs, J. (2015). Working with First Nation, Inuit and Métis families who have experienced family violence: A practice guide for child welfare professionals. Retrieved from http://cwrp.ca/sites/default/files/publications/en/FN_Inuit_Metis_Famili...
- Rivers, J. E., Maze, C. L., Hannah, S. A., & Lederman, C. S. (2007). Domestic violence screening and service acceptance among adult victims in a dependency court setting. Child Welfare, 86(1), 123-144. Retrieved from http://go.galegroup.com/ps/i.do?p=AONE&u=lond95336&id=GALE|A159645352&v=2.1&it=r&sid=summon&authCount=1
- Rizo, C. F., & Macy, R. J. (2011). Help seeking and barriers of Hispanic partner violence survivors: A systematic review of the literature. Aggression and Violent Behavior, 16(3), 250-264. doi: 10.1016/j.avb.2011.03.004
- Robinson, A. L., & Tregidga, J. (2007). The perceptions of high-risk victims of domestic violence to a coordinated community response in Cardiff, Wales. Violence Against Women, 13, 1130-1148. doi:10.1177/1077801207307797
- Rosenfeld, R. (1997). Changing relationships between men and women: A note on the decline in intimate partner homicide. Homicide Studies, 1, 72-83. doi: 10.1177/1088767997001001006
- Rothman, E. F., Gupta, J., Pavlos, C., Dang, Q., & Coutinho, P. (2007). Batterer intervention program enrollment and completion among immigrant men in Massachusetts. Violence Against Women, 13(5), 527-543. doi: 10.1177/1077801207300720
- Royal Canadian Mounted Police (RCMP). (2015). Missing and murdered Aboriginal women: 2015 Update to the national operational overview. Retrieved from RCMP website http://www.rcmp-grc.gc.ca/wam/media/455/original/c3561a284cfbb9c244bef57...
- Rural Health Information Hub. (2016). Conducting rural health research, needs assessment, and program evaluation. Retrieved from https://www.ruralhealthinfo.org/topics/rural-health-research-assessment-...
- Rying, M. (2001). Acts of lethal violence against women in intimate relationships (BRA report 2001:11). Stockholm, SE. Retrieved from https://www.bra.se/download/18.cba82f7130f475a2f1800027927/1371914734814...
- Sabri, B., Campbell, J. C., & Dabby, F. C. (2015). Gender differences in intimate partner homicides among ethnic sub-groups of Asians. Violence Against Women, 22, 1-22. doi:10.1177/1077801215604743
- Saez-Betacourt, A., Lam, B. T., & Nguyen, T. (2008). The meaning of being incarcerated on a domestic violence charge and its impact on self and family among Latino immigrant batterers. Journal of Ethnic & Cultural Diversity in Social Work, 17(2), 130-156. doi: 10.1080/15313200801941614
- Salcido, O., & Adelman, M. (2004). “He has me tied with the blessed and damned papers”: Undocumented-immigrant battered women in Phoenix, Arizona. Human Organization, 63(2), 162-172. Retrieved from https://www.lib.uwo.ca/cgi-bin/ezpauthn.cgi?url=http://search.proquest.c...
- Sam, D. L. (2006). Acculturation: Conceptual background and core components. In D. L. Sam & J. W. Berry (Eds.). Routledge Handbook of Acculturation Psychology (p. 11). Cambridge, UK: Cambridge University Press.
- Sandberg, L. (2013). Backward, dumb and violent hillbillies? Rural geographies and intersectional studies on intimate partner violence. Affilia, 28(4), 350-365. doi: 10.1177/0886109913504153
- Sandberg, L. (2013). Backward, dumb, and violent hillbillies? Rural geographies and intersectional studies on intimate partner violence. Affilia: Journal of Women and Social Work, 28, 350-365. doi: 10.1177/0886109913504153
- Saunders, D. G. (2007, October). Child custody and visitation decisions in domestic violence cases: Legal trends, risk factors, and safety concerns. National Online Resource Centre on Violence Against Women Retrieved from http://vawnet.org/sites/default/files/materials/files/2016-09/AR_Custody...
- Schilling, S., Snyder, A., & Scribano, P. V. (2012). Intimate partner violence: Pediatric risks of "not asking-not telling". Clinical Pediatric Emergency Medicine, 13(3), 229-238. doi:10.1016/j.cpem.2012.06.010.
- Schwartz, D. (2015, June 2) Truth and Reconciliation Commission: By the numbers. Retrieved from CBC News website: http://www.cbc.ca/news/indigenous/truth-and-reconciliation-commission-by...
- Shalabi, D., Mitchell, S., & Andersson, N. (2015). Review of gender violence among Arab immigrants in Canada: Key issues for prevention efforts. Journal of Family Violence, 30(7), 817-825. doi: 10.1007/s10896-015-9718-6
- Sharma, A. (2001). Healing the wounds of domestic abuse: Improving the effectiveness of feminist therapeutic interventions with immigrant and racially visible women who have been abused. Violence Against Women, 7(12), 1405-1428. doi: 10.1177/10778010122183928
- Sharma, A. (2007). Provision of domestic violence services for immigrant women: A case for re-examining the concept of cultural competence (Doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (UMI No. 3243425)
- Shea, B. N., Nahwegahbow, A., & Andersson, N. (2010). Reduction of family violence in Aboriginal communities: A systematic review of interventions and approaches. Pimatisiwin, 8(2), 35-60. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2970596/
- Sheikh, N. S. (2008). A matter of faith: Muslim women's perception of their faith community's response to intimate partner violence (Doctoral dissertation). Retrieved from ProQuest Dissertation & Theses Global. (UMI No. 3316939)
- Shepherd, J. (2001). Where do you go when it's 40 below? Domestic violence among rural Alaska Native women. Affilia, 16(4), 488-510. doi:10.1177/08861090122094389
- Shirwadkar, S. (2004). Canadian domestic violence policy and Indian immigrant women. Violence Against Women, 10(8), 860-879. doi:10.1077801204266310
- Shiu-Thornton, S., Senturia, K., & Sullivan, M. (2005). "Like a bird in a cage": Vietnamese women survivors talk about domestic violence. Journal of Interperssonal Violence, 20(8), 959-976. doi:10.1177/0886260505277677
- Shlonsky, A., & Friend, C. (2007). Double jeopardy: Risk assessment in the context of child maltreatment and domestic violence. Brief Treatment and Crisis Intervention, 7(4), 253-274. doi:10.1093/brief-treatment/mhm016
- Short, L. M., & Rodriguez, R. (2002). Testing an intimate partner violence assessment icon form with battered migrant and seasonal farmworker women. Women Health, 35(2-3), 181-192. doi: 10.1300/J013v35n02_12
- Sigal, J. I. (n.d.). Domestic Violence and Honor Killings. Retrieved from https://www.apa.org/international/united-nations/janet-sigal.pdf
- Sillito, C. L., & Salari, S. (2011). Child outcomes and risk factors in U.S. homicide-suicide cases 1999–2004. Journal of Family Violence, 26(4), 285-297. doi:10.1007/s10896-011-9364-6
- Silva-Martínez, E. (2016). "El silencio": Conceptualizations of Latina immigrant survivors of intimate partner violence in the Midwest of the United States. Violence Against Women, 22(5), 523. doi: 10.1177/1077801215607357
- Silverman, J. G., Mesh, C. M., Cuthbert, C. V., Slote, K., & Bancroft, L. (2004). Child custody determinations in cases involving intimate partner violence: A human rights analysis. Amerian Journal of Public Health, 94(6), 951-957. doi:10.2105/AJPH.94.6.951
- Singh, P. K. (2005). The Multicultural Partner Abuse Short Term Program: MPAST (Unpublished master’s thesis). Retrieved from ProQuest Dissertations & Theses Global.
- Sinha, M. (2013). Measuring violence against women: Statistical trends. Juristat, Statistics Canada Catalogue no. 85-002-X. Retrieved from http://www.statcan.gc.ca/pub/85-002-x/2013001/article/11766-eng.htm
- Social Development Committee of the Parliament of South Australia. (2016, April 12). Report into domestic and family violence: Thirty ninth report of the social development committee (Second session fifty-third parliament). Adelaide, SA: Parliament of South Australia.
- Sokoloff, N. J. (2005). Domestic violence at the intersections of race, class, and gender: challenges and contributions to understanding violence against marginalized women in diverse communities. Violence Against Women, 11(1), 38-64. doi:10.1177/1077801204271476
- Sokoloff, N. J. (2008). Expanding the intersectional paradigm to better understand domestic violence in immigrant communities. Critical Criminology, 16(4), 229-255. doi:10.1007/s10612-008-9059-3
- Sokoloff, N. J. (2008b). The intersectional paradigm and alternative visions to stopping domestic violence: What poor women, women of color, and immigrant women are teaching us about violence in the family. International Journal of Sociology of the Family, 34(2), 153-185. Retrieved from http://www.jstor.org/stable/23070750
- Sokoloff, N. J., & Dupont, I. (2005). Domestic violence at the intersections of race, class, and gender: Challenges and contributions to understanding violence against marginalized women in diverse communities. Violence Against Women, 11, 38-64. doi: 10.1177/1077801204271476
- Sokoloff, N. J., & Dupont, I. (2005). Domestic violence at the intersections of race, class, and gender: Challenges and contributions to understanding violence against marginalized women in diverse communities. Violence Against Women, 11, 38-64. doi: 10.1177/1077801204271476
- Sokoloff, N. J., & Pearce, S. C. (2011). Intersections, immigration, and partner violence: A view from a new gateway—Baltimore, Maryland. Women & Criminal Justice, 21, 250-266. doi: 10.1080/08974454.2011.584468
- Spath, R. (2003). Child protection professionals identifying domestic violence indicators: Implications for social work education. Journal of Social Work Education, 39(3), 497-518. Retrieved from https://www.lib.uwo.ca/cgi-bin/ezpauthn.cgi?url=http://search.proquest.c...
- Spiwak, R. (2004). Violence against separated women in Canada (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (MQ97192).
- Stanley, N., & Humphreys, C. (2014). Multi-agency risk assessment and management for children and families experiencing domestic violence. Children and Youth Services Review, 47(1), 78-85. doi: 10.1016/j.childyouth.2014.06.003
- Stanley, N., Miller, P., & Richardson-Foster, H. (2012). Engaging with children's and parents' perspectives on domestic violence. Child & Family Social Work, 17(2), 192-201. doi:10.1111/j.1365-2206.2012.00832.x
- Stanley, N., Miller, P., Richardson-Foster, H., & Thomson, G. (2010). Children and families experiencing domestic violence: Police and children’s social services’ responses. Retrieved from NSPCC website: https://www.nspcc.org.uk/globalassets/documents/research-reports/childre...
- Stanley, N., Miller, P., Richardson-Foster, H., & Thomson, G. (2011). Children's experiences of domestic violence: Developing an integrated response from police and child protection services. Journal of Interpersonal Violence, 26(12), 2372-2391. doi: 10.1177/0886260510383030
- Stansfield, R. & Williams, K. R. (2014). Predicting family violence recidivism using the DVSI-R: Integrating survival analysis and perpetrator characteristics. Criminal Justice and Behavior, 41, 163-180. doi: 10.1177/0093854813500776
- Statistics Canada. (2001). Rural and small town Canada: Analysis bulletin., Statistics Canada, Catalogue no. 21-006-XIE. Ottawa, ON. Retrieved from http://www.statcan.gc.ca/pub/21-006-x/21-006-x2001003-eng.pdf.
- Statistics Canada. (2006). Measuring violence against women. Statistical trends 2006. Statistics Canada. Catalogue no. 85-570-XIE. Ottawa, ON. Retrieved from http://www.statcan.gc.ca/pub/85-570-x/85-570-x2006001-eng.pdf
- Statistics Canada. (2008). Family violence in Canada: A statistical profile, 2008. Statistics Canada. Cat. no.85-224-x. pp.1-53. Ottawa, ON. Retrieved from http://ywcacanada.ca/data/research_docs/00000040.pdf.
- Statistics Canada. (2015). Family violence in Canada: A statistical profile, 2013.Statistics Canada, Catalogue no. 85-002-X. Ottawa, ON. Retrieved from http://www.statcan.gc.ca/pub/85-002-x/2014001/article/14114/section02-en...
- Statistics Canada. (2016a). Family violence in Canada: A statistical profile, 2014. Statistics Canada, Catalogue no. 85-002-x. Ottawa, ON. Retrieved from http://www.statcan.gc.ca/pub/85-002-x/2016001/article/14303-eng.pdf
- Statistics Canada. (2016b). Population centre and rural area classification 2016. Statistics Canada. Ottawa, ON. Retrieved from http://www.statcan.gc.ca/eng/subjects/standard/pcrac/2016/introduction#s3
- Stewart, L. A., & Power, J. (2014). Profile and programming needs of federal offenders with histories of intimate partner violence. Journal of Interpersonal Violence, 29(15), 2723-2747. doi:10.1177/0886260514526059
- Stöckl, H., Devries, K., Rotstein, A., Abrahams, N., Campbell, J., Watts, C., & Moreno, C. G. (2013). The global prevalence of intimate partner homicide: A systematic review. The Lancet, 382(9895), 859-865. doi: 10.1016/ S0140-6736(13)61030-2
- Stokes, V.M. (2012). Help-seeking in rural mothers who have experienced intimate coercive control in northwest Iowa: A phenomenological qualitative study (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertations &Theses Global. (UMI No. 3517572)
- Sullivan, M., Senturia, K., Negash, T., Shiu-Thornton, S., & Giday, B. (2005). "For us it is like living in the dark": Ethiopian women's experiences with domestic violence. Journal of Interpersonal Violence, 20(8), 922-940. doi:10.1177/0886260505277678
- Sutton, D., & Dawson, M. (2017, January). Femicide of older women. learning network Brief 31. London, ON: Learning Network, Centre for Research and Education on Violence Against Women and Children. Retrieved from www.vawlearningnetwork.ca/femicide-older-women
- Taft, A. J., Small, R., & Hoang, K. A. (2008). Intimate partner violence in Vietnam and among Vietnamese diaspora communities in Western societies: A comprehensive review. Journal of Family Studies, 14(2-3), 167-182. doi: 10.1080/15562948.2013.801734
- Tailor, K., & Letourneau, N. (2012). Infants exposed to intimate partner violence: Issues of gender and sex. Journal of Family Violence, 27, 477-488. doi: 10.1007/s10896-012-9441-5
- Taylor, R., & Jasinski, J. L. (2011). Femicide and the feminist perspective. Homicide Studies, 15, 341-362. doi: 10.1177/1088767911424541
- Thandi, G. S. (2013). A tale of two clients: criminal justice system failings in addressing the needs of South Asian communities of Surrey, British Columbia, Canada. South Asian Diaspora, 5(2), 211-221. doi: 10.1080/19438192.2013.740227
- Thibodeau, S., & Nixon, G. (2013). Transformation for Native men with assaultive issues: The medicine wheel and Wilber's spectrum of consciousness - A case study. The Canadian Journal of Native Studies, 33(1), 197-216. Retrieved from https://search.proquest.com/docview/1498366011?pq-origsite=gscholar
- Thomas, K. A., Goodman, L., & Putnins, S. (2015). "I have lost everything": Trade-offs of seeking safety from intimate partner violence. American Journal of Orthopsychiatry, 85, 170-180. doi: 10.1037/ort0000044
- Thurston, W. E., Roy, A., Clow, B., Este, D., Gordey, T., Haworth-Brockman, . . . Lesley, C. (2013). Pathways into and out of homelessness: Domestic violence and housing security for immigrant women. Journal of Immigrant & Refugee Studies, 11(3), 278-298. doi: 10.1080/15562948.2013.801734
- Trijbetz, T. (2011). Domestic and family violence and people from immigrant and refugee backgrounds. Retrieved from http://www.mhima.org.au/pdfs/Domestic%20and%20family%20violence_fact%20s...
- Turner, W., Broad, J., Drinkwater, J., Firth, A., Hester, M., Stanley, N., . . . Feder, G. (2015). Interventions to improve the response of professionals to children exposed to domestic violence and abuse: A systematic review. Child Abuse Review, 26(1) doi: 10.1002/car.2385
- Tutty, L. M. (2006, August). Effective practices in sheltering women leaving violence in intimate relationships (Phase II report 2006) . Retrieved from YWCA Canada website: http://ywcacanada.ca/data/publications/00000013.pdf
- Ulbrich, P. M., & Stockdale, J. (2002). Making family planning clinics an empowerment zone for rural battered women. Women & Health, 35, 83-100. doi: 10.1300/J013v35n02_06
- UNICEF Canada (2011). Proposed amendment to immigration and refugee protection regulations: Introduction of ‘conditional’ permanent residence period for spousal and partner sponsorships. Retrieved from http://ccrweb.ca/files/unicef-conditionalprstatus.pdf
- UNICEF. (2011). Manual for the measurement of indicators of violence against children. Retrieved from https://www.unicef.org/violencestudy/pdf/Manual%20Indicators%20UNICEF.pdf
- United Nations Office on Drugs and Crime. (2013). Global study on homicide 2013: Trends, contexts, data. Retrieved from https://www.unodc.org/documents/data-and-analysis/statistics/GSH2013/201...
- Urbanski, K. (2001). Counseling in shelters for Aboriginal women (Unpublished doctoral dissertation). Retrieved from ProQuest Dissertations & Theses Global. (MQ65174)
- Van Dyke, N. F. (2005). Domestic violence: Differences among rural, urban and suburban women (Unpublished doctoral dissertation). State University of New York at Binghamton, Binghamton, NY.
- Van Hightower, N. R., & Gorton, J. (2002). A case study of community-based responses to rural woman battering. Violence Against Women, 8, 845-872. doi: 10.1177/107780102400388506
- Van Hightower, N. R., Gorton, J., & DeMoss, C. L. (2000). Predictive models of domestic violence and fear of intimate partners among migrant and seasonal farm worker women. Journal of Family Violence, 15, 137-154. Retrieved from https://link.springer.com/article/10.1023/A:1007538810858
- Varcoe, C., & Dick, S. B. (2008). The intersecting risks of violence and HIV for rural Aboriginal women in a neo-colonial Canadian context. Journal of Aboriginal Health, 4(1), 42-52. doi:10.1177/019394599701900403
- Varcoe, C., & Irwin, L. G. (2004). “If I killed you, I'd get the kids”: Women's survival and protection work with child custody and access in the context of woman abuse. Qualitative Sociology, 27(1), 77-99. doi: 10.1023/B:QUAS.0000015545.82803.90
- Vaughan, C., Davis, E., Murdolo, A., Chen, J., Murray, L., Block, K., . . . Warr, D. (2015). Promoting community-led responses to violence against immigrant and refugee women in metropolitan and regional Australia: The ASPIRE Project (State of knowledge paper 7). Australia National Research Organisation for Women’s Safety, 12, 1-81. Retrieved from http://media.aomx.com/anrows.org.au/s3fs-public/12_1.2%20Landscapes%20ASPIRE%20web.pdf
- Vaughan, C., Murdolo, A., Murray, L., Davis, E., Chen, J., Block, K., Quiazon, R., & Warr, D. (2015). ASPIRE: A multi-site community-based participatory research project to increase understanding of the dynamics of violence against immigrant and refugee women in Australia. BMC Public Health, 15, 1-9. doi: 10.1186/s12889-015-2634-0
- Victorian Indigenous Family Violence Task Force. (2003). Victorian Indigenous Family Violence Task Force final report. Retrieved from http://www.deadlyrav.com.au/assets/Uploads/2016-update/vic-indigenous-fa...
- Vidales, G. T. (2010). Arrested justice: The multifaceted plight of immigrant Latinas who faced domestic violence. Journal of FamilyVviolence, 25(6), 533-544. doi: 10.1007/s10896-010-9309-5
- Vishnuvajjala, R. (2012). Insecure communities: How an immigration enforcement program encourages battered women to stay silent. Boston College Journal of Law & Social Justice, 32(1), 185-213. Retrieved from https://www.lib.uwo.ca/cgi-bin/ezpauthn.cgi?url=http://search.proquest.c...
- Vives-Cases, C., Torrubiano-Dominguez, J., Gil-Gonzalez, D., La Parra, D., Agudelo-Suarez, A. A., Davo, M. C., & Martinez-Roman, M. A. (2014). Social and immigration factors in intimate partner violence among Ecuadorians, Moroccans and Romanians living in Spain. J Public Health, 24(4), 605-612. doi: 0.1093/eurpub/ckt127
- Wachter, K., & Donahue, K. (2015). Bridge to safety: An evaluation of a pilot intervention to screen for and respond to domestic violence and sexual assault with refugee women in the U.S. Technical Report. doi: 10.13140/RG.2.1.3643.3369.
- Washington State Coalition Against Domestic Violence. (2011). Immigrant and refugee victims of domestic violence homicide in Washington state. Retrieved from https://wscadv.org/wp-content/uploads/2016/12/immigrant-victims-dvfr-iss...
- Wathen, C. N., & MacMillan, H. L. (2013). Children's exposure to intimate partner violence: Impacts and interventions. Paediatrics & Child Health, 18(8), 419-422. doi: 10.1093/pch/18.8.419
- Wathen, C. N., & MacMillan, H. L. (2013). Children's exposure to intimate partner violence: Impacts and interventions. Paediatrics & Child Health, 18(8), 419-422. doi: 10.1093/pch/18.8.419
- Waugh, F., & Bonner, M. (2002). Domestic violence and child protection: Issues in safety planning. Child Abuse Review, 11(5), 282-295. doi: 10.1002/car.758
- Weisz, A. N., Tolman, R. M., & Saunders, D. G. (2000). Assessing the risk of severe domestic violence: The importance of survivors’ predictions. Journal of Interpersonal Violence, 15, 75-90. doi: 10.1177/088626000015001006
- Weizmann-Henelius, G., Matti Grönroos, L., Putkonen, H., Eronen, M., Lindberg, N., & Häkkänen-Nyholm, H. (2012). Gender-specific risk factors for intimate partner homicide: A nationwide register-based study. Journal of interpersonal violence, 27(8), 1519-1539. doi: 10.1177/0886260511425793
- Welland, C., & Ribner, N. (2010). Culturally-specific treatment for partner-abusive Latino men: A qualitative study to identify and implement program components. Violence and Victims, 25, 799-813. doi: 10.1891/0886-6708.25.6.799
- Wells, L., Strafford, B., & Goulet, S. (2011). Shift: The project to end domestic violence – Research in the Calgary Aboriginal community. The Centre for Criminology and Justice Research. Retrieved from https://www.edmontonsocialplanning.ca/index.php/resources/digital-resour...
- Wendt, S. & Hornosty, J. (2010). Understanding contexts of family violence in rural, farming communities: Implications for rural women’s health. Rural Society, 20, 51-63. doi: 10.5172/rsj.20.1.51
- Wendt, S., Buchanan, F., & Moulding, N. (2015). Mothering and domestic violence: Situating maternal protectiveness in gender. Affilia Journal of Women and Social World, 30(4), 533-545. doi:10.1177/0886109915570925
- West Coast Legal Education and Action Fund (LEAF). (2012). Position paper on violence against women without immigration status*. Retrieved from http://ccrweb.ca/files/position_statement_-_women_without_status_leaf.pdf
- West, C. M. (2015). African immigrant women and intimate partner violence: A systematic review. Journal of Aggression, Maltreatment & Trauma, 1-14. doi: 10.1080/10926771.2016.1116479
- Wider Opportunities for Women. (,2013, April). Rural survivors & economic security. (Population policy series). Retrieved from http://www.wowonline.org/wp-content/uploads/2013/05/ESS-Population-Polic...
- Williams, K. R. (2012). Family violence risk assessment: A predictive cross-validation study of the domestic violence screening instrument-revised (DVSI-R). Law and Human Behavior, 36, 120-129. doi:10.1037/h0093977
- Williams, K. R., & Grant, S. R. (2006). Empirically examining the risk of intimate partner violence: The revised domestic violence screening instrument (DVSI-R). Public Health Reports, 121, 400-408. Retrieved from http://journals.sagepub.com/doi/pdf/10.1177/003335490612100408
- Williams, K. R., & Houghton, A. B. (2004). Assessing the risk of domestic violence reoffending: A validation study. Law and Human Behavior, 28, 437-455. doi: 10.1023/B:LAHU.0000039334.59297.f0
- Wisniewski, A., Arseneault, R., & Paquet, M. (2016). Rural realities faced by service providers and women survivors of intimate partner violence when navigating the justice system. Retrieved from https://www.unb.ca/fredericton/arts/centres/mmfc/_resources/pdfs/ruralre...
- Wolf, M. (2015). Barriers to adequate services for rural victims of domestic violence (Unpublished master’s thesis). Winona State University, Winona, MN. Retrieved from https://www.winona.edu/counseloreducation/media/rural%20victims.pdf
- Wolfe, D. A., Crooks, C. V., Lee, V., McIntyre-Smith, A., & Jaffe, P. G. (2003). The effects of children's exposure to domestic violence: A meta-analysis and critique. Clinical Child and Family Ppsychology Rreview, 6(3), 171-187. Retrieved from https://link.springer.com/content/pdf/10.1023%2FA%3A1024910416164.pdf
- World Health Organization (WHO). (2012). Intimate Partner Violence. Retrieved from http://apps.who.int/iris/bitstream/10665/77432/1/WHO_RHR_12.36_eng.pdf
- World Health Organization (WHO). (2012). Understanding and addressing violence against women. Retrieved from http://apps.who.int/iris/bitstream/10665/77432/1/WHO_RHR_12.36_eng.pdf
- World Health Organization (WHO). (2016). Global plan of action to strengthen the role of the health system within a national multisectoral response to address interpersonal violence, in particular against women and girls, and against children. Retrieved from http://apps.who.int/iris/bitstream/10665/252276/1/9789241511537-eng.pdf?...
- World Health Organization (WHO). (2002). Violence - A global public health problem. In E. G. Krug, L. L. Dahlberg, J. A. Mercy, A. B. Zwi, & R. Lozano (Eds.). World Report on Violence and Health (pp.1-19). Geneva, CH: World Health Organization.
- Yang, M., Wong, S. C., & Coid, J. (2010). The efficacy of violence prediction: A meta-analytic comparison of nine risk assessment tools. Psychological Bulletin, 136, 740-767. doi: 10.1037/a0020473
- Yick, A. G., & Oomen, E. (2009). Using the PEN‐3 model to plan culturally competent domestic violence intervention and prevention services in Chinese American and immigrant communities. Health Education, 109(2), 125-139. doi:10.1108/09654280910936585
- Yoshihama, M. (2001). Immigrants-in-context framework: Understanding the interactive influence of socio-cultural contexts. Evaluation and Program Planning, 24(3), 307-318. doi: 10.1016/S0149-7189(01)00021-0
- Yoshihama, M. (2002). Battered women's coping strategies and psychological distress: Differences by immigration status. American Journal of Community Psychology, 30(3), 429-452. Retrieved from https://link-springer-com.proxy1.lib.uwo.ca/content/pdf/10.1023%2FA%3A10...
- Yoshihama, M., Blazevski, J., & Bybee, D. (2014). Enculturation and attitudes toward intimate partner violence and gender roles in an Asian Indian population: implications for community-based prevention. American Journal of Community Psychology, 53(3-4), 249-260. doi:10.1007/s10464-014-9627-5
- Young, H. L., Mancuso, A. F., Faherty, E., Dorman, S. A., & Umbrell, J. R. (2008). Helping child victims of family violence through school personnel: An evaluation of a training program. Journal of Aggression, Maltreatment & Trauma, 16(2), 144-163. doi:10.1080/10926770801921386
- Yuan, N. P., Belcourt-Dittloff, A., Schultz, K., Packard, G., & Duran, B. M. (2015). Research agenda for violence against American Indian and Alaska Native women: Toward the development of strength-based and resilience interventions. Psychology of Violence, 5(4), 367-373. doi: 10.1037/a0038507
- Zannettino, L. (2012). “. . . There is no war here; it is only the relationship that makes us scared”: Factors having an impact on domestic violence in Liberian refugee communities in South Australia. Violence Against Women, 18(7), 807-828. doi:10.1177/1077801212455162
-
Zarza, M. J., & Adler, R. H. (2008). Latina immigrant victims of interpersonal violence in New Jersey: A needs assessment study. Journal of Aggression, Maltreatment & Trauma, 16(1), 22-39. doi: 10.1080/10926770801920453
- Zellerer, E. (2003). Culturally competent program: The first family violence program for Aboriginal men in prison. The Prison Journal, 83(2), 171-190. doi: 10.1177/0032885503083002004
- Zink, T. (2000). Should children be in the room when the mother is screened for partner violence? Journal of Family Practice, 49(2), 130-130. Retrieved from http://go.galegroup.com/ps/i.do?p=AONE&u=lond95336&id=GALE|A60039856&v=2.1&it=r&sid=summon
- Zorn, K. G., Wuerch, M. A., Faller, N., & Hampton, M. R. (2017). Perspectives on regional differences and intimate partner violence in Canada: A qualitative examination. Journal of Family Violence. Advance online publication. doi: 10.1007/s10896-017-9911-x
[1] The researchers chose to review literature published as early as 2000 as the start of a new century yet current enough to capture changes in policies and practices around domestic homicide prevention. The review ends in 2015, when the literature review began.
[2] A software tool for managing bibliographies, citations, and references.
[3] For example, Heise (1998) identifies four levels of the framework (personal history, microsystem, exosystem, and macrosystem), and Oetzel and Duran (2004) identify five levels (intrapersonal/ individual, interpersonal, institutional/organizational, and policy).
* The Danger Assessment is also considered an actuarial tool in its current form.
[4] The CDHPIVP includes all victim-focused strategies to manage risk in its definition of safety planning (see below).
[5] Indigenous peoples, formerly referred to as Aboriginal, includes the Indian, Inuit, and Metis peoples of Canada (Section 35, Constitution Act, 1982).
* The article by Marchetti and Anthony (2016) was not included in the literature review but is cited to provide context on the international perspective of legal strategies adopted by mainstream courts to facilitate collaboration with Indigenous peoples.
[6] Table citations: Annan, 2008; Averill, Padilla, & Clements, 2007; Barton, Hungler, McBride, Letourneau, & Mailloux, 2015; Banman, 2015; Beyer, Layde, Hamberger, & Laud, 2013; Bosch & Bergen, 2006; Bosch & Schumm, 2004; Coy, Kelly, Foord, & Bowstead, 2011; Choo, Newgard, Lowe, Hall, & McConnell, 2011; Doherty & Hornosty, 2004; Doherty & Hornosty, 2008; Eastman & Bunch, 2007; Eastman, Bunch, Williams, & Carawan, 2007; Edwards, Mattingly, Dixon, & Banyard, 2014; Evanson, 2006; Faver & Strand, 2003; Grama, 2000; Hornosty & Doherty, 2002; Kasdorff & Erb, 2010; Logan et al., 2003; McCall-Hosenfeld, Weisman, Perry, Hillemeier, & Chuang, 2014; Owen & Carrington, 2015; Peek-Asa et al., 2011; Van Hightower & Gorton, 2002; Wolf, 2015.
[7] In this study, “rural” includes areas with a population under 30,000.
[8] Placating strategies are “private attempts to impact the abuser’s behavior without challenging his control” and resistance strategies are “private attempts to impact the abuser’s behavior by challenging his control” (Anderson et al., 2014, p. 430).
[9] In immigrant and refugee populations, domestic violence may not be limited to intimate partners, male intimate partners may not be the primary or sole perpetrators, and incidents of domestic violence or homicide may involve multiple perpetrators and victims/survivors, including extended family members.
[10] Dynamic risk factors have the potential to shift and change. Unlike static risk factors that can be used to predict instances of domestic violence and assess risk (e.g., perpetrator’s history of violence), dynamic risk factors are potential foci of intervention strategies.